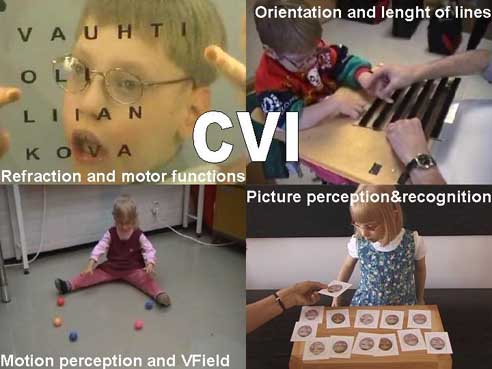
Organisation of CVI Assessment

This unusually crowded cover slide depicts the confusion that nearly everybody feels in trying to cover the assessment of vision of children with CVI. This one-day course in San Francisco was originally planned to be for a small group but on the day of the lectures we were more than 150. Since I needed to describe many aspects of CVI writing notes and studying the numerous slides simultaneously would not have worked. Therefore the slides are here on my homepage for further discussion and for preparation of the five webcast that are planned for next year, starting just before the AAPOS meeting in March.
This time I will write less than usually under the slides hoping that the participants of the course, and also other readers, will comment and ask questions.
The central questions were these usually less discussed special features of CVI: Videos are not on this homepage material. They will be in the webcast and will be clearer than they would be on this homepage. I plan to make them available also on a DVD. In many observations video documentation is essential to confirm that the impression that we had while working with the child is correct. Sometimes we find several other features in a child’s functioning when we analyse the videos over and over again.
- oculomotor problems including accommodation
- motion perception and visual field
- recognition functions from perceptions of details in visual information to recognition of facial features.
Please, refer to the text Visual Perception tests in Paediatric Vision Tests and to the text in the beginning of the
Cognitive Vision Tests, the Introduction to the LEA Cognitive
Vision Tests.



This diagram was originally drawn for the EPOG conference in 1983 to stress the fact that during communication
and assessment we need to pay attention to a great number of nonvisual factors that may affect use of vision.


To demonstrate the great variation of functioning in children with CVI, I showed a few slides of four children.
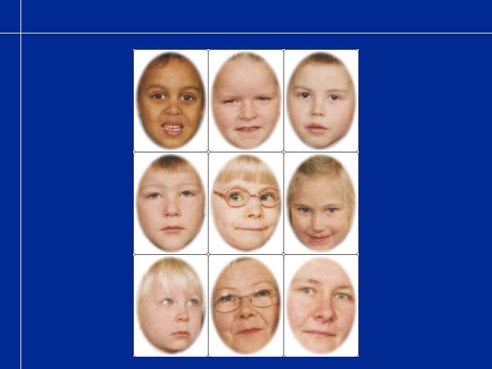
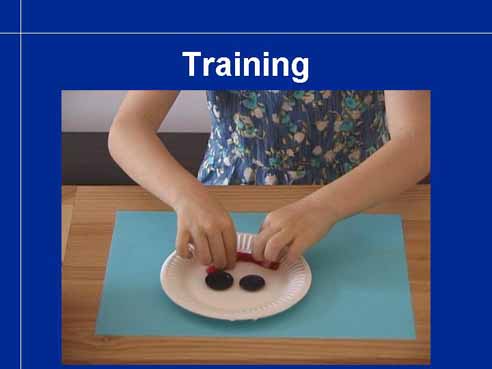
Recognition of facial features may be totally lost so that not even the family members and other significant persons are recognised by their faces but voice, clothing, jewellery, way of moving etc. It is necessary to test whether there is a poor quality image that makes recognition difficult or whether there is good quality image but it cannot be connected with a template in memory, become re-cognised.
By making test cards of each child’s closest friends, family members and teacher carefully avoiding other information but the face on the cards, we can test whether the child can match, find pairs of similar pictures. In this case that was no problem. Yet the child did not know who are the persons in the pictures. First when she was told that the persons presented in the cards were all in her day care group, she deduced that the child with the glasses must be she herself because she is the only one who has glasses.


Perception of facial expressions is socially equally important as recognition of faces. Therefore it is of utmost importance
to assess visibility and perception of facial expressions as early as there are any suspicions on the infant�s ability to
participate in visual communication.

There is a small special group of children with severe motor problems including inability to speak but with extremely sharp
and well functioning image analysis. Many people would claim that these children are not visually impaired. That is not really
true because they have losses in spatial visual functions; perception of surface qualities and nearly every one of them requires
consultation by an experienced teacher for visually impaired. Since use of visual information is limited by the motor problems,
presentation of it needs to be planned specifically for each child using the techniques that the child can use to activate a computer.
Auditory functions need to be assessed as carefully as those of a blind child and auditory teaching materials modified to the child�s
needs.
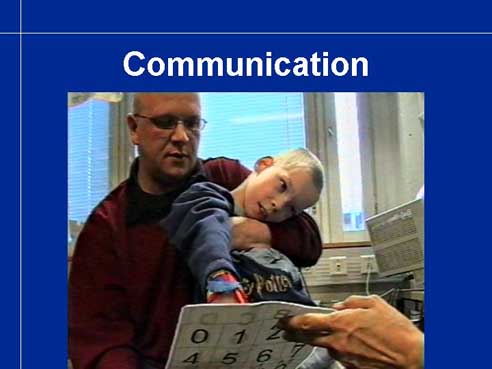
This first slide shows this boy pointing on the correct color cap using a stick fixed on his wrist. Note that the end of the stick
is covered with soft cotton material so that the stick will not scratch the surface of the caps.
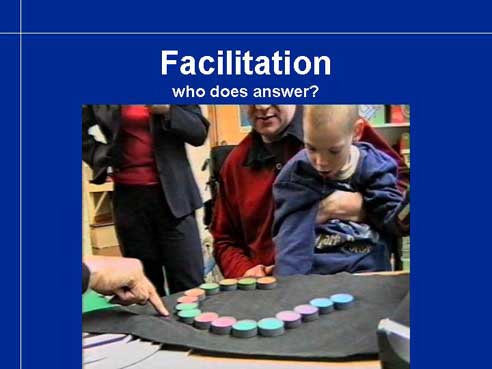
When a child can perform the arm movements only by being facilitated by an adult, the question often is �Who is the one who
responds, the child or the adult?� In this case it was very clear that it must be the child who performed normally in the color vision test.
His father had typical red-green deficiency and could by no means help his son in color vision tests.
(This is not the result that the father had but a more severe deficiency that I described to the team.)

The ability of these children to read a whole page by letting the eyes glide across the page is always surprising. After having briefly looked on the cover of an old phone directory (old so that he couldn’t know it) and asked where there is a name he pointed to it without hesitation.
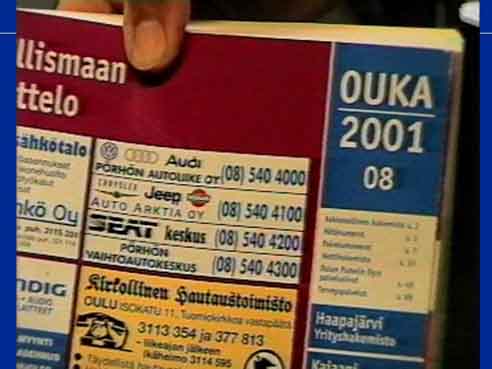
The name in small print is the first name under the numbers 08 in the right upper corner.
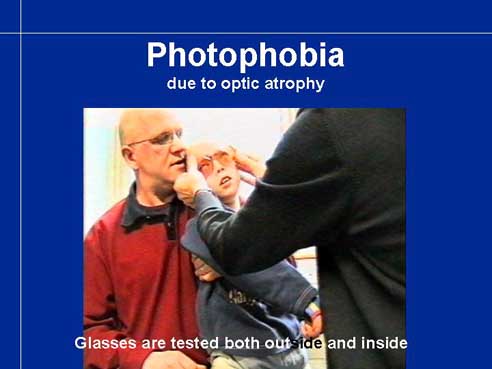
Children with optic atrophy nearly always have photophobia caused by the change in rod-cone-interaction. It can be
prevented by choosing a filter lens that reduces transmission in bluegreen part of spectrum, the part that the rod cells are sensitive to.
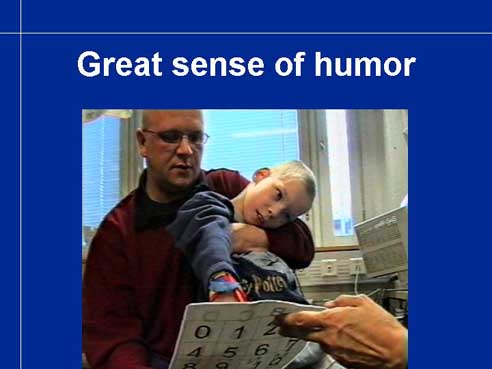
These children often impress by their great sense of humour and positive self-image despite the seemingly impossible life situation. This boy wrote a humorous compliment when I had demonstrated the filter lenses and explained how they work. The statement clearly showed that he felt himself equal to the adult persons present with full rights to be different.
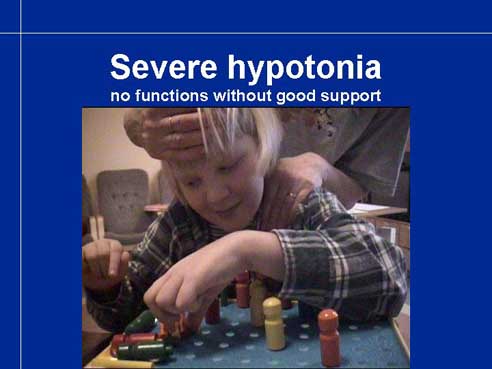
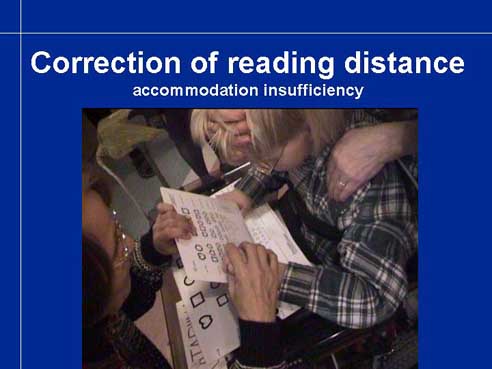
Another often-misunderstood group of children are those with extreme hypotonia like this girl who cannot get her head up from the desk without support. When supported, she enjoys age appropriate tests and even adjusts test distance during near vision testing to correspond to her insufficient accommodation by pushing the test to a longer distance.


Children with rare syndromes may have limited losses of higher visual functions as well as motor problems. Since the effect of a deletion of a part of a chromosome varies from child to child, assessment needs to be repeated twice a year to learn which visual functions develop age appropriately and which do not appear as expected and require compensatory techniques. Assessment is often complicated by the fact that we know equally little about the development of hearing and ability to hear speech as speech, not only as sounds. There may be also numerous other deviations from normal development in all functional areas. However, it is possible to measure a few important variables and observe the use of vision so that the early intervention team has some useful information to start with.



Children with CVI are often described as children with severe intellectual disabilities. There are those children, too and their assessment is so difficult that I have not found a way to teach the assessment techniques with lectures. Each child is a challenge to the early intervention team and the assessment requires years of observation by the teachers and therapists to develop communication.
The great majority of children with CVI function well in many areas, some children are very high functioning with amazing
linguistic abilities even if they are unable to speak.
In the assessment of children with CVI we need to remember the fact that is true to all visually impaired children:
they experience the world different from normally sighted and therefore have a different framework for development
of all functions. This is not so different as one may think, because each of us experiences the world individually
and there is no way of knowing how another person perceives the world. It is important that we do not use our world
as the measure stick when assessing or helping children to learn but try to get glimpses of their world and help them
to find ways to use different modalities in effective ways, yet maintaining the playful atmosphere of childhood.