
Lecture in St.Petersburg on November 1.2002
Spectacles and training are the two most common treatments of amblyopia and strabismus. If children's vision screening occurs early, most children can be treated with conservative treatment, spectacles and training and thus few children need to be operated. If treatment is well organised the number of visits at the ophthalmologist's office does not need to be more than a few and we spare both time and money and the child develops good vision in both eyes.
During this short introduction to discussion I have chosen to discuss only esotropia, the most common deviation from normal alignment treated before school age. In its earliest stage it may present as a delay of development of accommodation. It can be detected if an infant does not have a normal eye contact that the parents experience as a difficulty in interaction. In its mildest form the baby is felt to have "dreaming eyes", i.e. not a usual, sharp eye contact but otherwise good interaction. If these infants are referred at the age of 3-4 months and found not to accommodate, it is possible to help their interaction with spectacles.

Figure 2. At the age of four months this baby girl turned her head away when an adult tried to interact with her. This was interpreted as a sign of infantile autism. Since two of the older three siblings had esotropia, the infant was referred for an examination. She had normal looking eyes, a refractive error of +1.0 I both eyes and no accommodation to accommodative targets. Therefore +4.0 lenses were placed in front of her eyes to give her a clear image on the retinas. The effect was immediate, the baby looked surprised and a few seconds later showed a normal social smile for the first time.
The infant in slide 2 was referred to my office at the age of 4 months. A young general practitioner made the diagnosis "infantile autism" because the infant "avoided eye contact". Next to the infant stands her brother who had been treated for esotropia. The experienced health care nurse recommended referral, especially, since two of the three older siblings had esotropia. The clearly unusual behaviour of the infant is obvious in the video (in the CD: LH Materials 2001/ Accommodation). The video was taken two weeks after the examination at the health care centre. Since the infant did not seem to be able to bring her gaze to midline, I asked the mother to bring the hands of the infant to the midline. This often helps to use vision in midline. In this case it did not.
During examination she was found to have a refractive error of +1.0 in both eyes and no accommodation to accommodative targets. Therefore glasses +4.0 were tried and immediately the infant could use her vision in midline, looked surprised when looking at her mother and then - for the first time - showed a typical social smile.
I tease my colleagues neurologists saying that +4.0 lenses are the most effective way to treat infantile autism. There is some truth in this statement. Some infants and young children, who have problems in developing communication, may have specific vision impairments as the basic cause of their problems. Therefore, whenever an infant does not have normal active interaction with the parents, visual functions need to be evaluated, also accommodation.
There were no other pathologic findings and the infant had been found healthy, so the family borrowed a pair of +4.0 lenses in COMO-frames. I suggested that they would use the glasses during communication most of the time during the first week and then increase the time without glasses. I also warned them that many children with a delay in use of accommodation later develop esodeviations.

Figure.3. A combination of optic penalisation and bifocal correction was needed to keep the eyes aligned both when looking at distance and at near.
Two months later the parents called telling that the right eye had started to turn in. Since there was so little basic hyperopia, the right eye was overcorrected three dioptres and the left one diopter. This proved not be enough at near. Since she had only slight esophoria with her +4.0 lenses, the left lens was made bifocal. With this correction her eyes were aligned most of the time and she developed even some stereovision.
 Figure 4. At the age of six years the girl has her eyes aligned when using her glasses with a near lens for the right eye and a progressive lens for the left eye.
Figure 4. At the age of six years the girl has her eyes aligned when using her glasses with a near lens for the right eye and a progressive lens for the left eye.
At the age of three years the girl developed overaction of the inferior oblique muscle; however, it was present only when the glasses were not worn. She is now six, with the glasses her eyes are aligned. She has lost her weak stereovision but is still binocular in Worth's and Schober's test and her visual acuity is normal in both eyes.


Figure 5. This infant had had infantile spasms and strong medication. She was mostly very sleepy and did not look at people or objects. When her lacking accommodation was compensated with near correction she immediately had eye contact with me.
Insufficient or absent accommodation is common in infants with infantile spasm or hypotonia of their muscles, as was the case with this infant. The eyes may at this age be aligned but the infant looks through you rather than at you. Correction with glasses that compensate for the lack of accommodation is important so that the infant can have better interaction with his/her parents. As you can see in the corresponding video (in CD: LH Materials 2001/ Accommodation), there can be a momentary change in the infant's behaviour when glasses are used. Such a marked change does not occur in every case; sometimes glasses need to be used during communication and feeding for several days before the infant becomes interested in interaction and in objects around. In this group of children strabismus varies. It is treated with glasses and when necessary short time patching, one to two hours a day, to teach the child to use both eyes. Surgical treatment is usually postponed as long as the child has strong medications that affect motor control and wakefulness.
Anisometropia is another common cause for treatment with glasses and training. There are two different groups of children with anisometropia:
- those with congenital difference in refraction and
- those whose emmetropisation occurs in unequal amounts in the two eyes leading to anisometropia at the age of 3-6 years.
Since these children often have normal looking eyes and the eyes are aligned, refractive difference and amblyopia is often diagnosed quite late. If amblyopia developes late, at the age of four - five years, the child may notice it him- or herself.
In the congenital form binocularity may develop if the infant is examined early, the refractive error corrected and the eye at risk is trained. The difference in refraction is sometimes so great that correction with a contact lens is the only possibility to have good enough image quality by reducing the size difference.

Figure 6. Esotropia of the left eye and 5 dioptres of difference in refraction at the age of 4 years is likely to be due to asymmetric emmetropisation because visual acuity became nearly symmetric after correction of the refractive error and a few weeks of training.
The girl in this slide has typical late onset anisometropia. Her eyes had looked normal until she developed esotropia at the age of four years. At that time visual acuity of the left eye was 0.05 without correction and 0.25 with correction. With full correction and training of the left eye visual acuity became equal to that of the right eye (0.8) but there was still esotropia of the left eye. Such an amblyopia is likely to be of late onset.
Schober's test often helps in the diagnostic assessment of children with anisometropic amblyopia. The test picture contains two green rings and a red cross. When viewed through red - green lenses a binocular person sees both the rings and the red cross. If there is a phoria, the cross moves corresponding to the angle of phoria.
If the child sees the rings when the green lens is in front of the amblyopic eye but not the cross when the red lens is in front of the amblyopic eye, the area of suppression of the image of that eye is very small, the size of the cross.
Figure 7. Schober's test. If suppression of the amblyopic eye is weak, the cross may be seen "blinking".
Sometimes the child tells that (s)he sees the cross "blinking", i.e the cross appears for a short time and then disappears again for a short time. In such a case suppression is weak and can usually be broken in a short time. Since we usually do not have follow-up visits sooner than a month, it is not possible to know how soon the function became normal. If the child has intensively trained the amblyopic eye, visual acuity may become normal within a month. Training must be both fun and demanding; nowadays many children like to play different electronic games, the smaller, the better. Nokia's phone is useful also in this regard; the "Worm"-game is an excellent training game.

Figure 8. Explaining the use of a copy of the near test in training for measurement of visual acuity during the next visit.
We usually think of training as training of fixation and training of visual acuity. Training of the test symbols and responding is important in the assessment of young children so that visual acuity can be tested as early as possible. In the two-year old children, near testing is easier that testing at a distance of three meters, so a copy of the near vision test is given as homework. I give a copy of the side with larger symbols when I expect that the child will see the smaller symbols after training. The parents can use the test first at the usual 40cm distance and then at 80cm and 120cm distance.

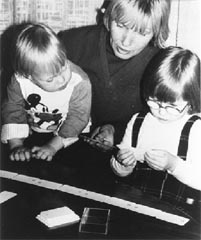
Figure 9. Training for vision testing at an early age. The concepts 'same' and 'different' need to be learned in terms of colour and then form so that visual acuity can be measured with optotype tests.
Children under the age of two years may start the training with the 3D LEA Puzzle to develop the concepts "similar" and "different" first in terms of colours and then in terms of forms. The next step is to learn to place the correct puzzle piece on a flat picture of similar size of each symbol, then on smaller and smaller symbols, at which time we are testing visual acuity with single symbols.
When an older sibling has been found to have an amblyopic eye, the younger siblings are examined in most countries. If an infant has similar refractive error as the child with amblyopia, we want to teach the infant to respond in the test situation as early as possible. If the infant is watching the older sibling training with the  Domino, the symbols become familiar and even the names may be learned early. Until visual acuity can be measured, we must rely on our observations on the quality of fixation, signs of stereovision, prism test and other common clinical test situations.
Domino, the symbols become familiar and even the names may be learned early. Until visual acuity can be measured, we must rely on our observations on the quality of fixation, signs of stereovision, prism test and other common clinical test situations.
The Domino was designed for training of amblyopia at a time when visual acuity is 0.63 or better and there are few pictures that are small enough to train visual acuity further. The smallest symbols (.32M corresponding to 1.25 at 40cm) of the LEA Domino are difficult to see even by a normally sighted adult person.


Figure 10. Poor and good fitting of spectacles.
In training of central vision, fitting the glasses is instrumental. Glasses that allow the child to look over, are of no use. These glasses do not have a "saddle"-type nose piece, which should preferably be of silicon so that it does not glide on the small nose. In Finland we have often difficulties with fitting, because our infants and young children have no nose between their eyes and they have high check bones. In some cases we have had to construct extra thickness in the "saddle" by using the material that dental technicians use for the gums of the prosthesis.
Patching is a constant matter of discussion. The variation of patching is much the same in many countries. From the mildest to the total occlusion, the stages in my use are:
1. cover of the lower lens with Bangerter's Einschleich occlusion, translucent film,
2. cover of the lower lens with opaque occlusion.
These are common when the eyes are aligned and we do not want to disturb binocularity. The amblyopic eye often has near correction so we are using a combination of penalisation and occlusion.
3. Full Einschleich occlusion,
4. full opaque occlusion
5. Opticlude or similar glued on occlusion, sometimes pirot's patch, when occlusion is of short time during a game.
A less common occlusion is optic occlusion of +5 to +7 diopters in case of nystagmus.

Figure 11. Effective occlusion by using soft facial tissue to cover the leading eye during training or testing.
We can also use a soft tissue to have full occlusion during training. This type of full occlusion many young children accept better than occlusion on the lens or a glued on occluder. I have chosen this picture of a three year old girl with Down Syndrome to start and to end my lecture to stress the fact that many children with amblyopia and strabismus are to be found among children with other impairments, especially among children with intellectual disabilities and children with motor problems. If a child cannot yet do demanding near work we can start with drawing for the child asking the child for advice how to draw, so that the child holds fixation at the tip of the pencil.
These aspects are those I wanted to discuss. Several of these practises are well known, some might be new. I would be very much interested in the opinions of my collegues on the use of spectacles and training in treatment of strabismus and amblyopia. The e-mail address for comments is lea.hyvarinen@lea-test.fi