Visual Field
Among all clinical tests the results of usual visual field measurements of deaf patients are the least reliable. The reason quite apparently is inadequate communication because deaf patients are visually more alert than hearing persons and likely to perform exceptionally well in vision tests, if they know what their response should be.
Tests for the measurement of visual field are the regular tangent screen and Goldmann perimetry or automated perimetry with minor modifications. If the clinical examination is started with careful measurement of confrontation fields for "communication field" and that information is given to the laboratory, we usually get repeatable results. Another cause for variation in the size of visual fields is visual adaptation. If the patient is tested after different periods of adaptation to room light the size of the field varies in many cases of retinal degeneration. When visual fields are measured for research purposes it is essential that exposure to bright light prior to the measurement is carefully avoided for several hours.
Use of the perimeter tests requires explanation of the test situation to the interpreter. If both the interpreter and the patient are new, it is advisable to demonstrate the test by first briefly measuring the visual field of the interpreter. This gives the patient an opportunity to observe what is going on and it makes the test situation much easier for the interpreter to describe. In retinitis pigmentosa, Goldmann perimetry is often a lot easier than the automated perimetric tests because the flickering, spontaneous lights that these patients see are hard to distinguish from the small flashing lights of the automated perimeter.

|
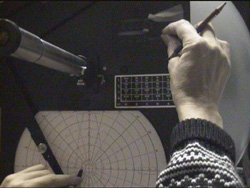
A. The child is shown how one makes the marks when there is a response from the person tested, first in the periphery and... |
|

|
B. ...then in the middle. |
|
|
C. The size of the stimulus lights can be changed on the tester's side; the child also goes to the other side to confirm that the light changes. |
|
|
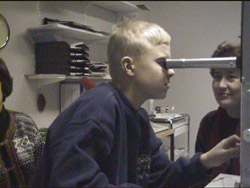
D. The child looks through the tube to find out that it is possible to see the eye of the person on the other side of the instruments. |
|

|
E. Finally the child can try to move the stimulus while observing the eye of the person to be tested. (A short video on these sequencies is on the LH Materials 2001 CD.) |
There are no widely accepted guidelines on how we should measure the visual field in retinitis pigmentosa. The difference in the size of the isopters IV/4 (or V/4) and 1/4 is a measure of the loss of retinal function at low photopic luminance levels. The area of visual field that does not respond normally to the 1/4-stimulus is, as a coarser sieve, unable to capture finer details of visual information.
The size of a ring scotoma should be roughly estimated in the office prior to laboratory tests. This otherwise difficult measurement is easier if we know approximately what we are looking for. Quite often deaf patients are unaware of the structure of their visual field and have unnecessary worries about their vision because objects disappear and reappear in midperiphery. This question was included in the teaching tape with the hope that it would be explained regularly in the future.
Examination of Goldmann field in young deaf children requires a skilled technician and plenty of time. When I examine the fields myself, which I do if there are any difficulties, the first fields are of no use, the second fields measured a few weeks later gave a general idea about the structure of the field and the third fields measured again a few weeks or months later can be rather reliable. However, it is my experience that the isopters, measured in Goldman perimetery, often tend to grow between 6 and 9 years of age although it is more likely that there is slow constriction. This means that the child learns to communicate with us better and also concentrates better in the test situation.
If the patient has a small tubular field, it is easier to assess using regular white paper at 57 cm distance, or at 114 cm if the field is very small. At 57 cm, one centimetre on the surface is equal to one degree of visual angle. The patient fixates on a cross in the middle of the paper and responds when he sees the black target, a simple black pen, coming from the side. This may sound unsophisticated, but the field measured with this technique is closely equal to the IV/4-isopter of the Goldmann fields. The size of the field in degrees is equal to the size of the area seen, measured in centimetres.
Some patients experience changes in the size of the visual field at different luminance levels. In order to record this we can measure visual field first on a white surface (usually at 30-50 cd/m2), then on a black surface (somewhere around 1-4 cd/m2) and finally on a lightbox with a 200 cd/m2 luminance level. The size of the field may be exactly the same in all of these three conditions or it may vary by becoming smaller both at low and high luminance levels or only at a low luminance level.
Visual fields and legal blindness
There seems to be considerable confusion among the parents and teachers of Usher youngsters regarding the size and quality of the visual field. Since these children would not otherwise get the services they need, it often seems that the size of the visual field is reported as being smaller than it actually is so that the child can be classified "legally blind". This is a sad and counterproductive situation that needs to be changed. Decisions related to eligibility for services should be made by experts in the field of deafblind rehabilitation, and should not be based on a single number. The present practice unfortunately leads to very strange situations. For example, children with beginning ring scotoma, when the 1/4-isopter is still 60-80 degrees in diameter, are given cane instruction for daylight mobility. The child, who can see may get a very distorted idea of him- or herself, not understanding why he is being taught cane techniques. In some cases the child's resistance in not accepting the cane has made the teacher and parents talk about the ensuing blindness so much that the child becomes afraid of losing his sight in near future.
One of the corner stones of rehabilitation is that the patient is taught what he has to live with. Without this knowledge he cannot be in charge of planning his future. Parents and teachers must also get accurate information in a form they can understand and use in everyday situations. It is very difficult to explain the structure of the visual field in detail, but most often the explanation given in our teaching videotape is quite satisfactory as the first round of information. Understanding makes the patient and the parents more alert, since the more they know, the more they are likely to remember and report observations and be eager for more information and explanations from the doctor.
Figure 10. Blinking stimulus that can be turned on and off is a good test target for confrontation field and as an introduction of visual field testing. This device was produced at the University of California, Berkeley, School of Optometry.
Central scotoma
Central scotoma is often ill defined, patchy, the image distorted and discoloured. A good assessment of this visual problem is not easy to achieve. The use of the Amsler grid as the first test is particularly useful when examining deaf patients since it is rather easy to explain and it can be done by the patient over and over again while waiting for other tests.
If the regular Amsler test does not reveal central scotoma but there is metamorphopsia of the image, testing in reduced illumination, at a level where the grid can barely be seen, may demonstrate the scotomas better. This can be done by using a dimmer or, if reproducible test conditions are needed, by using cross-polarizing filters.
An exact measurement of the size and configuration of central scotoma on a tangent screen requires good fixation. It is facilitated by using a cross similar to that used in the Amsler grid.
Assessment of visual field in young and low functioning patients
Normally sighted deaf children are usually very alert to visual information in their peripheral vision. Test objects that appear from behind the patient are noticed quickly. The test situation is the same as that used when examining normally sighted, hearing children. If the child is old enough to respond to the wand moving within the visual field, it is helpful first to show the child that the blinking light can be turned off. Then the wand is moved back and forth in an area of the visual field which is likely to function normally. The light is turned on and off and the child is requested to sign "yes" every time the light blinks. In this way we learn how good an observer the child is. When this part of the test is successfully completed, we can start examining other areas of the visual field, again asking the child to answer each time the light blinks. The very same technique is used in the office examination of many adults as an introduction to Goldmann or automated visual fields.
When we measure the visual field in low functioning, multidisabled children, there are numerous sources of errors. The observations on the size of the visual field should always be made in a play situation where the child or the adult is at an optimal activation level. If the cognitive development is below 6 months of age, lack of attention to peripheral information may reduce the apparent size of the visual field as it does in normal infants during the first few months of life.
![]()
![]()
![]()