Important First and Preschool Years in the Development of Vision
In most countries there is a tradition of recording the structure of the eyes, red reflex and the ocular motor functions at birth and a few times during the first year to detect cataract, glaucoma, and strabismus but development of vision is usually recorded only once as “good eye contact” at 6 weeks, latest at 8 weeks of age. However, often the infant with poor visual communication is not immediately referred for examination by an ophthalmologist, the family is asked “to wait and see”. The recent Manual for Health Care Centres in Finland (2011) there are several ages, at which vision should be specifically observed and at each of the nine visits during the first year, the quality of eye contact and the red reflex should be recorded.
Specific ages for follow-up of vision development of healthy children in basic health care:
- Birth: structure of the eyes, red reflex, strabismus
- 6 - 8 weeks: good eye contact
- 12 weeks - 4th month: - active visual communication, hands found
- baby follows lip and hand movements of children and adults
- fixation, following movements, convergence develop steady
- 7 - 8 month: pincer grasp, face recognition, Hirschberg
- 18 month: face recognition, Hirschberg, cover test (H+ct)
- 3 year: (H+ct), near vision acuity
- 4 year: (H+ct), near and far vision acuity
- 5 year: if visual perceptual problems >> ophthalmologist first; the psychologist’s examination later when the child has used glasses a few weeks. During the examination the child uses glasses.
Whenever the parents are worried about the infant’s visual behaviours, the infant needs to be referred to an ophthalmologist who is accustomed to assess infants and young children.
Infants with a greater than usual risk of having vision disorder:
- small prematurely born infants
- newborn infants with asphyxia
- newborn deaf or hard of hearing infants (Retinitis pigmentosa)
- infants with hypotonia, later developing spasticity
- infants with high hyperopia or weak accommodation
- infants with Down syndrome or intellectual disability
- infants with a syndrome known to include vision disorders
- twins
- after accidents and infections
Most of these infants are in the hospital care so they should be easy to detect if the personnel is aware of these well-known risk groups. After the first year these same children are the largest groups of vision impaired children with new symptoms and signs developing later in the preschool years.
Questions on vision development at different ages:
The questions at different ages are related to important observations at each age of the child. The observations at birth have been recommended such a long time that midwifes and doctors seldom miss obvious deviations from the normal/typical development.
Vision is a central function in the development of communication, interaction and bonding during the first year. Visual information makes the infant aware of her/his body; body awareness is the beginning of awareness of space and moving and thus central in motor development. Therefore all visually impaired, even otherwise healthy infants need supporting therapy in communication and motor development. Deviations from normal visual communication or motor development should always make us ask whether the infant’s vision is developing normally.
Development of vision is fastest during the first year and therefore also deviations from normal development can and should be noticed early.
At the age of 2 months all typically developing infants with normal, enjoyable interaction with the parents have good eye contact and often also a social smile. It should develop during the third month at the latest. Both eye contact and social smile are important for the development of bonding. If an infant has weak accommodation or several dioptres of farsightedness, the eye contact may look as if the infant looked through the parent, which is experienced so unpleasant that parents mention it to health care personnel. These infants need to be examined by an ophthalmologist without delay to receive their eye glasses (spectacles) so that their visual communication and interaction can develop normally.
In many countries these young infants with poor near vision are not referred to an ophthalmologist and even if they are examined by an eye doctor their accommodation is rarely assessed and the infant is not given eye glasses, which leads to failing in visual communication due to the blurred double images (no accommodation, no convergence). How many of these children develop secondary autism and never have normal interaction, has not been studied. We meet children with uncorrected or partially corrected high hyperopia and autistic behaviours at school age with the history of no visual communication during early infancy when emotional bonding usually develops based on visual communication and interaction.
An infant with failing visual communication should be carried in sling or arms and sung and talked with to compensate for the loss of visual bonding. This also helps parents to learn to communicate with their baby and prevents depression, which is a common problem in the parents who do not experience normal eye contact and social smiles. Baby gymnastics and massage are good activities to support motor development and interaction in the family. See the Leo Video.
An infant and his/her parents need training and support in developing communication and interaction if the glasses do not immediately make the infant’s visual communication normal. A referral to paediatric neurologist is needed to evaluate possible atypical brain functions, especially if the infant is even slightly hypotonic. (Hypotonia and large refractive errors are common in infants with Down syndrome; also hypotonic infants who later develop spasticity may have hypotonia of intraocular muscles and therefore weak accommodation.)
In hearing impaired and deaf infants the possibility of Usher syndrome should be known. Since severe hearing defects are diagnosed at birth, early diagnosis of Usher syndrome is possible by asking about double sensory loss in extended family and in most countries genetic diagnosis is available.
 B.
B.C.

Figure 1. New-born baby watches the expressions of her mother intently and succeeds in copying some basic expressions on her second day of life, even a smile (A and B). This means that she must 1) perceive the expressions, 2) create an internal image of them, which is then 3) used as a map for planning of motor functions and 4) can execute the motor functions, not perfectly but so that we can see the similarity between the expressions on the mother’s face and on the infant’s face. New-born infant’s vision functions much better than the responses to full contrast gratings reveal. Visual function uses low contrast images in motion, i.e. facial expressions and other environmental movements at intermediate and low contrasts. C. At the age of 8 weeks a normally sighted baby can communicate with both parents shifting attention between them.
Questions during the health care visit:
| Question 1: | Do you have an enjoyable eye contact with your baby? Yes __, No __ |
| Question 2: | When you smile, does your baby immediately respond to your smile? Yes __, No __ |
| Question 3: | When you smile, does your baby respond with a smile first when you say something? Yes __, No __ |
| Question 4: | Does your baby watch the mobile moving above her/his bed? Yes __, No __ |
| Question 5: | Do you have a feeling that your baby looks through you when you hold the baby at less than a foot distance from your face? Yes __, No __ |
| Question 6: | Is the communication with your baby stressful in any way? Yes __, No __ |
| Question 7: | Do you have concerns or worries about the eyes or vision of your baby? Yes __, No __ |
| Question 8: | Does anyone in your extended family have vision or eye problems? Yes __, No __ |
If any of the “red flags” is noticed, discuss problems related to birth, any symptoms of asphyxia and refer the infant first to an ophthalmologist with specific questions on accommodation, convergence and refraction. If these are found normal, consultation of a paediatric neurologist is important to investigate why the brain functions do not use the visual information that seems to be normal at the level of the eyes.
If there is/are persons with atypical vision or known diseases in the family, an eye doctor needs to be consulted on whether the infant should be examined or only followed for certain signs. If a condition is rare and not known by the doctor, the specialists of genetic and other rare diseases should be consulted so that there is no delay in early intervention for infants with rare disorders.
At the age of 4 months the infants have usually noticed their hands at the age of 3 months, have brought them to the midline (an important milestone in motor development and body awareness) and into the mouth (gives the baby concrete information on the form and movements of hands). Watching and playing with hands strengthens stereo vision.
The baby is also starting to keenly watch lip movements and movements of hands of parents and children, first hits and then grasps toys hanging above, and moves a lot. If the baby is visually impaired, motor development and visual interaction show delay. Infants with “mild brain damage” (i.e. few motor problems, perhaps a little difficulty with head control or body control) may have so poor visual awareness of space that they are afraid to be left alone and cling to their parents. They need the tactile contact to feel safe, like blind infants.
The questions used at 2 months of age can be repeated and seven new questions are suggested.
A. 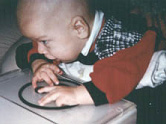
B. 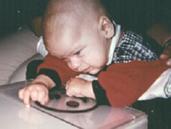
 C.
C.
Figure 2. This infant with normal eyes had not noticed his hands and had not started playing with them at the age of four months. A. Therefore he was observed when the hands were placed on a visuo-tactile picture, i.e. the black forms were cut out of black plastic (edges rounded) and glued on clear plastic that was placed on a lightbox. B. When the hand happened to touch a tactile line, he watched his hand for the first time with wrinkles on his forehead. C. To have confirming tactile information about the visual “something” he brought his hands into his mouth for the first time.
Questions during the health care visit:
| Question 1: | Did your baby notice her/his hands a few weeks ago? Yes __, No __ |
| Question 2: | Does she/he watch her/his hands moving them in different positions? Yes __, No __ |
| Question 3: | Does she/he bring the hands to the midline and into the mouth? Yes __, No __ |
| Question 4: | Does your baby notice you approaching at a distance of a few meters and greet you with a smile when you smile? Yes __, No __ |
| Question 5: | Is your visual interaction with your baby rich and enjoyable? Yes __, No __ |
| Question 6: | Does she/he have good head control when on tummy? Yes __, No __ |
| Question 7: | Does your baby demand to be carried by you more than other infants? Yes __, No __ |
Again, answers marked with red require further questioning and assessment by a paediatrician and/or paediatric neurologist. If an ophthalmologist has not examined the infant, then ophthalmological examination should be arranged prior to the paediatric or neuropaediatric examination to exclude high refractive errors and problems in accommodation. Question 7 is related to the situation that the infant has undiagnosed brain damage that prevents development of body awareness that in turn is crucial in understanding the space around. An infant may therefore not want to be alone at all and clings to the parents and other adults as if they were the center of the universe. Such an infant should be carefully examined and observed because if the infant does not recognize where he or she is, being left alone causes a stress situation that negatively affects the development of brain. All other symptoms and signs of “mild” brain damage should be documented and treated as a part of early intervention.
If an infant is diagnosed to have some delay in motor development, helping the infant to see hands and feet by bringing them close to the eyes, watch face in a mirror, and experience his body during baby massage are easy activities to arrange and widen the infant’s visual sphere and thus entice the infant to explore his/her surrounding world. Special playmats with good contrasts function as the first maps for orientation in space and exploration of little spaces creates the awareness of using reaching and grasping to “grasp the world”.
The first six months are an important period of development of many brain functions related to mirror neuron system. At the age of 4 to 5 months it is advisable to observe whether these early visual and motor functions have developed in a typical way:
- eye contact
- social smile and visual interaction
- emotional bonding
- noticing own hands and exploring them
- keen observation of movements of lips of adults
- bringing hands to midline and into mouth
- copying of goal-directed hand movements of other children and adults
Four month old infants are vividly aware of parents’ emotional state and, for example, experience the beginning depression of the mother so frightening that they turn away from visual communication with the mother. This happens before the medical specialists have become aware of the mother’s depressive moods and should be used in the observation of communication of healthy infants with their parents.
All infants receive information on weight, size, and surface qualities of objects by exploring them with their hands and mouth. This gives the concrete structure to the more abstract “visual something”. The explorations need to be repeated over and over again to result in a multimodal engram or concept in the memory that later gets a name as a word or a sign. Passive stimulation by showing pictures and videos without allowing the infant to explore is empty entertainment and does not lead to learning.
Observing and copying goal-directed hand movements of other children and adults and starting to copy them is an important milestone. Individual variation in the milestones is related to the experiences of infants. Some infants are surprisingly dexterous in building towers because parents, usually the father or older siblings have shown how to build with blocks and explained what they were doing. Infants and their parents enjoy play situations where they can watch and copy other infants hand movements like the little artists in the pictures below.


Figure 3. The Art Museum in Pori was the first place in Finland to arrange painting sessions where the very young artists have an opportunity to watch other infants’ activities in painting and copy their hand movements. This play situation is also fun to watch by the parents or caregivers.
At the age of 6 months the baby loves to copy activities of other babies and children, observes the environment, watches people eating, and, especially, interaction between parents and other people as if checking whether the other people are friends with the parents. This sometimes develops to a fear when meeting new people at the age of 8 months (even family members whom the infant has not seen in a week, especially if hair is covered and cloths are different from previous contact).
The infant now recognizes his bottle or cup and favourite toys. At this age eyes should be “straight”, ortophoric. Eye-turn in or out may occur when the infant is close to falling asleep. Strabismus developing at this age should be assessed without delay because correct glasses may help the infant to remain binocular and even develop good stereovision without patching or surgery (Fig. 4). Suddenly developing strabismus may sometimes, but rarely, be caused by a tumor growing into the central retina and destroying sharpest vision, so that the eye cannot be aligned with the healthy eye. In such a case the child’s eyes need to be examined with no delay.



Figure 4. A. This infant’s strabismus developed when she was 6 months old. In these pictures she is nearly 8 months old. She had first usual bifocal glasses with large reading section (like the left eye’s lens) and was ortophoric through the reading sections but the right eye was in inward squint when looking through the distance section of the lens and thus the infant saw double images. Therefore the right lens was changed to reading lens that blurred the image at distance (= distance penalization) and the child did no more see double. Vision could develop normally without patching or surgery.
Questions during the health care visit:
| Question 1: | Is visual communication with your baby enjoyable. Yes __, No __ |
| Question 2: | Are the eyes of your baby looking at the same target? Yes __, No __ |
| Question 3: | There is no eye turn in or outwards except when falling asleep? True __, Not true __ |
| Question 4: | Is your baby using her/his toys like other infants? Yes __, No __ |
| Question 5: | Is your baby watching other children’s play? Yes __, No __ |
| Question 6: | Does your baby watch the surrounding people and places? Yes __, No __ |
At this age the parents could be suggested buying (or using older children’s) building blocks and playing with them in front of the infant telling that the adult is “placing this red block (or brick) on this other blue block to make a tower”. Similarly the concept of categories can be built using the everyday objects mentioning their names when for example placing cutlery on the table.
If there is even the slightest worry about visual functions, support visual learning with tactile, auditory and movement information. Touch your face with the infant’s hands, in play situations strengthen the experiences of spatial structures and body awareness, and ask for thorough functional assessment of your infant.
(For further information see www.lea-test.fi,
at the address http://www.lea-test.fi/en/assessme/lowvisio/index.html)
At the age of 8 to 12 months the differences in developing motor functions become greater than earlier and therefore some of the functions may be present first close to the first birthday.
Eye-hand coordination develops so that the infant starts to poke on tiny crumbs on the floor at about 8 months and then develops pincer grasp. In the test situation we use cake decoration sweets on light surface. The dark tiny sweets measure detection vision at high contrast and the light coloured sweets detection at lower contrast levels. There must be sufficient vision in at least in one eye to notice the small sweets. Whether vision of the two eyes is symmetric, is difficult to test because at this age many infants are not easily enticed to watch something so that the eyes can be covered in turn. However, it is possible to observe at home when the baby is communicating with a parent while the other parent covers the line of vision of one eye in turn without touching the face. (Fig. 5)
A. 
B. 
 C.
C.
Figure 5. “Cover test” at home: A. The line of sight of one eye is obstructed while the infant is watching mother talking. B. Mother moved closer to the camera while the other eye’s line of sight is obstructed. Since this happened while the mother was moving, the infants did not notice the change in the “cover”. C. If the infant is looking at something on the side, it may look like that an eye is squinting inwards (the left eye in this case) but this is an incorrect interpretation because both eyes have moved toward the child’s right.
Infants start to recognize objects that are partially covered. They start to notice the difference between family members and other people at the age of 5-7 months and recognition of the faces of family members is well developed at the age of 10-11 months. They recognize family members BEFORE these say something and greet them with a big smile. If family members are not recognized, infant’s eyes need to be examined. If they are normal, a paediatric neurologist is consulted on higher visual functions. There is a risk that an infant with difficulties in face recognition is diagnosed as having “autistic behaviours”. If ever you hear anyone using this expression “autistic behaviours” about your infant or child, require a thorough examination of vision for communication so that the child’s communication difficulties are correctly interpreted.
Questions during the health care visit:
| Question 1: | Does your baby have pincer grasp? Yes __, No __ |
| Question 2: | Does your baby recognize known objects that are partially covered? Yes __, No __ |
| Question 3: | Does your baby recognize family members before hearing their voice? Yes __, No __ |
| Question 4: | Is her/his reaction to unknown people somewhat serious/ worried? Yes __, No __ |
| Question 5: | Does your baby play Hide and seek? Yes __, No __ |
| Question 6: | Does your baby 1) enjoy his baby books or 2) does she/he turn the pages only? 1. __ 2. __ |
At the age of 10 to 12 months, infants love to play hide and seek and know their way around in their home. They can look out of the window and recognize people. They also start to recognize some pictures. They still put everything into mouth to explore but also learn to explore objects banging them
(http://www.lea-test.fi/en/vistests/pediatric/vactests/mysight/whatic.html).
Some very alert infants observe adult persons’ functions, especially eating and may point with a finger to some dish that everyone seems to like using a demanding sounding “a” “a” – a function that we may observe at the age of 5 months but usually first at the age of 10 to 12 months.
At the age of 18 months, typically developing infants with normal motor functions move at lot, walk and start to run; eye-hand coordination is sufficient for eating with baby-spoon and fingers. If the infant has high hyperopia and sees everything blurred at close distances, he keeps running from place to place to find something to play with and does not play with usual playthings like his peers. These children do not develop strabismus so their eyes look normal. Therefore their behaviour is interpreted as “hyperkinesia and attention deficit”. Both problems disappear momentarily when the infant gets proper glasses.
Normally sighted infants’ eyes are straight and they can use both eyes equally well. Cover test is still difficult but is often successful when the eyes are covered in turn with a cap (Fig.6 A and B). If playing continues unchanged when the eyes are covered in turn, vision in both eyes is likely to be equally useful for the infant’s activities (may not be quite the same).
A. 
B. 
 C.
C.
Figure 6. A and B. Covering eyes in turn may reveal that one eye is strongly preferred. C. This infant had been watching parents playing with blocks and puzzles already before her first birthday. She had herself played with puzzles from the age of 12 months. At the age of 18 months she “tells” her parents that she knows where the puzzle piece should be placed. This nine piece puzzle does not have color coding of the cut-outs; therefore it requires good form recognition and matching. Video
During communication visual information is fast moving shadows on the faces of parents and other adults.
Fear of small fast moving dogs is a first typical symptom of difficulties in motion perception; small dogs are seen as blurred balls that disappear and reappear and sometimes touch the infant.
Difficulties in motion perception affect fast, short lip movements. The mouth may look unpleasantly blurred so that the infant looks past the adult person’s face when listening.
When answering the child looks at the adults face. If the eye contact is not quite typical because of difficulties in focusing, the child may seem to look “through the adult’s head”. This atypical "behaviour" can be wrongly interpreted as “avoiding eye contact”.
Atypical features in visual communication should be assessed by a specialist team for children with problems in processing of visual information. If an infant is not properly assessed and has the words “autistic behaviours” in his report, they are very difficult to be removed. The child is not sent for assessment of vision from later examinations because his/her atypical visual behaviours will be interpreted “autistic”.
This delays an early diagnosis of visual processing difficulties and causes inadequate early intervention.
Questions during the health care visit:
| Question 1: | Has the development of visual communication and interaction continued with normal milestones? Yes __, No __ |
| Question 2: | Has the motor development continued with normal milestones? Yes __, No __ |
| Question 3: | Does your infant recognize your close relatives and neighbors? Yes __, No __ |
| Question 4: | Does your infant play near other toddlers and watch their play? Yes__, No __ |
| Question 5: | Does your child tolerate covering of eyes in turn? Yes __, No __ |
| Question 6: | Is your infant afraid of small animals or objects moving fast? Yes __, No __ NOTE! |
| Question 7: | Is he/she happy to explore a playground or does it look frightening? Happy __, worried __. |
At the age of 20 to 26 months, normally sighted infants have developed an understanding of the concept “same” comparing first colours, slightly later forms. Using comparison between single test pictures (optotypes in LEA Playing Cards) and the LEA Puzzle pieces as the play, binocular visual acuity can be measured in many children. It is important to play quietly (hand clapping disturbs child’s concentration) and gently describe and confirm what the infant is doing: “Yes, that puzzle piece and the picture are the same”. “This puzzle piece is the same as this small picture.” Stop playing if the child loses interest in looking at the small pictures. Do NOT ask the child to “look more carefully” – that means forcing the child to function at too high a level.
A. 
 B.
B.
C. 
 D.
D.
Figure 7. Developing the concepts used in testing visual acuity. A. Matching “same colour”. B. Same black-and-white concrete form (Note that the child’s hand is rotated to a position ready to turn the puzzle piece into correct orientation before the child has grasped the puzzle piece = eye-hand coordination and awareness of directions are well developed). C. Concrete form on flat picture. D. Comparing concrete forms and tiny picture = measurement of visual acuity with small single optotypes at the age of 26 months.
Picture books are usually an important part of the day and the child is keen in learning new names of common animals, flowers, cars and objects in the household and around the house. When the child is given a new book it is wise to let the child tell what she/he sees in the book. It effectively depicts concept building and visual perception. Boys often surprise by recognizing cars in tiny pictures on newspapers’ “On Sale”-pages or at longer distances than their grandparents. They can start to recognize landmarks if these are discussed on the way to important places. - Playing with blocks reveals eye-hand coordination and the concepts of structures that can be built.
Many typicaly developing children want to be small helpers and participate in setting table and taking dishes back to the kitchen. Children with different disabilities are happy if there is something that can be their "work", even if it is only telling what should be done next. In the questions some No-answers can be due to motor disability and and not due to impaired vision. Also blind children can learn to bring their plate to kitchen.
Children with difficulties in perceiving facial expressions and body language (either the image is blurred or the specific cortical function has not developed) avoid playing with peers of same age because their ‘ranking order’ is defined by subtle visual behaviours that they are unaware of. Such a child stays with adults, often learns to talk quite early as a compensation for the difficulties in visual communication. Sometimes the social situation in a group of toddlers becomes better, if the infant’s processing disorder is hidden behind slightly darkened spectacles with side shields.
Typical behaviours of vision impaired toddlers look superficially like the behaviours of toddlers with autistic spectrum disorders without the child having any emotional or interaction problems with persons who understand the child’s communication. The child uses tactile and auditory information more than a sighted child to learn doors by the sounds of the hinges and locks and the surface structure and form of the door handle. This type of exploration requires numerous repetitions to recognise the subtle details. (For more information visit the lecture Autism and CVI.)
Questions during the health care visit:
| Question 1: | Can your child match colours, i.e. red and blue colours in different boxes? Yes__, No __ |
| Question 2: | Does he/she know body parts? Yes__, No __ |
| Question 3: | Does he/she feed him-/herself at the table? Yes__, No __ |
| Question 4: | Does he/she ‘help’ you in the household chores? Yes__, No __ |
| Question 5: | Can he/she pull socks off? Yes__, No __ |
| Question 6: | Can he/she help in getting dressed? Yes__, No __ |
| Question 7: | Does he/she play with other children taking turns and waiting? Yes__, No __ |
| Question 8: | Can he/she express him-/herself using words, gestures, body language? Yes__, No __ |
At the age of 27 to 36 months, infants with disabilities, like children with Down syndrome (Fig.8) and cerebral palsy can learn to participate in many test situations where visual functions for recognizing forms or daily tasks are assessed. The next step is to learn to accept cover in front of an eye and looking with one eye on small single pictures. Most children bend close to tiny pictures, which is a normal strategy at this age. Linear tests like the usual LEA Near Card, is difficult at this age. Some children have cognitive space (= visual sphere) for recognition of forms at 5 feet so that visual acuity can be measured as distance visual acuity with single symbols. If a child has the concept “in the middle”, his/her visual acuity can be measured with the smallest test with crowding symbols around the symbol in the middle.
A. 
 B.
B.
C. 
 D.
D.
Figure 8. Children with other disabilities should have had the opportunity to play with the test symbols for weeks so that the concept “same” is well developed. Half of infants and toddlers with Down syndrome has refractive errors and/or weak focusing power (accommodation) so that their glasses, which they should have had since the age of 3 or 4 months, need to be carefully checked before visual acuity values are measured.
Questions during the health care visit:
| Question 1: | Does your child have any of the common visible problems like cerebral palsy or Down syndrome. Yes __, No __ |
| Question 2: | Has his visual development been followed regularly. Yes__, No__ |
| Question 3: | Has his/her communication developed smoothly? Yes __, No __ |
| Question 4: | Does he/she have friends in the neighbouring houses and by your relatives. Yes __, No __ |
| Question 5: | Is he/she afraid when you go into dark places. Yes __, No __ |
At the age of three and half to four years, children in many countries have vision screening for late detection of amblyopia. Most cases of amblyopia have been diagnosed earlier, especially those related to strabismus. Also children in families with amblyopia in the older siblings or cousins have been tested for monocular visual acuity, fusion and stereovision as early as possible. Asymmetric visual acuity or unwillingness to use the other eye should prompt a consultation with the vision specialist who functions at the referral centre for amblyopia screening.
Some children with inherited retinal diseases may start to develop symptoms of “night blindness”. When we go into a darker place we first see poorly but then our sight becomes clearer, our eyes adapt to a lower luminance level. In some retinal diseases this adaptation time becomes longer at this age and children may ask to have a night light in their bedroom. Visual acuity and contrast sensitivity show normal values, visual field is of normal size. The only problem is the long adaptation time. The progression of changes is usually very slow and children learn to avoid dark places. CONE Adaptation time should be recorded for the follow-up of retinal changes and genetic study is advisable to learn about possible on-going treatment studies.
At the age of 42 to 48 months, children are often ready to the 4-year control of sensory and motor functions. At the age of four years, children’s ability to discriminate improves thus small visual objects and pictures close to each other can be recognized. The eye movements needed to fixate and move the gaze from one small picture to another on the visual acuity tests are better controlled. Some children, however, have irregular saccades, which require further examinations.
A. 
 B.
B.
C.
 D.
D.
Figure 9. A. For examination of each eye individually, one eye must be covered with a screening frame that does not disturb the child. B. Standard near test. C. Easy screening test for testing children who have difficulties in seeing details close to other details. D. Distance visual acuity tests.
Visual acuity values at a near distance (40 cm, 16 inches) and at a far distance (3 m, 10 feet) are binocularly 0.5, 6/12, 20/40 or better (i.e. same as the lowest visual acuity for traffic vision in adults) and in both eyes closely the same, i.e. the difference between visual acuity values is less than two test lines (Fig.9). You can observe eye functions also in play situations and compare with those of other children. If you notice behaviours that are different from the typical behaviours, discuss them with the paediatrician of the health care centre.
A. 
B. 
 C.
C.
Figure 10. Kindergartens include play situations that prepare children for the 4-year follow-up examination. A. Play situation to keep the Styrofoam ball floating above the ring is a good situation for observation of convergence, turning in of eyes symmetrically. At the same time the pupils become smaller. (Published by permission of Verena Petz.) B. LEA Puzzle is useful in development of the concept “same” that is needed in many test situations. C. Pointing where the test card can be placed is an easy, concrete way of answering.
Questions during the health care visit:
|
If the child has had several ear infections or other diseases with frightening experiences of medical people, the child needs to have the test situations in the nursery school or in the play area of the Children’s Hospital with an occupational therapist or a nurse. The test situations should be calm and gentle with no hurrying from one test to another.
At the age of 54 to 60 months, children are usually quick in visual tasks and easy in vision screening.
A child, who has visited an eye doctor at the age of 3-4 years and has been found to have normal sight and normal looking eyes may sometimes develop visual problems later. If a child’s results in vision screening, even when repeated, are considerably poorer (more than two test lines) than those obtained earlier, the possibility of very rare hereditary diseases should be considered. They cause a decrease in visual acuity and contrast sensitivity, neurological symptoms and changes in personality. Changes in the child’s personality often make assessment of vision difficult, which should be seen as a diagnostic feature rather than postponing the test until “the child co-operates”.
A thorough functional and educational assessment of visual functioning is needed before the child visits the paediatric ophthalmologist’s and paediatric neurologist’s office so that all functional areas have been discussed and a list of questions and observations is ready for reporting to the doctors.
Questions during the health care visit:
| Question 1: | Has your child’s day a regular structure and rhythm? Yes __, No __ |
| Question 2: | Is your child happy at the kindergarten? Yes __, No __ |
| Question 3: | Does he/she play with other children outside? Yes __, No __ |
| Question 4: | Is your child interested in books, puzzles and constructive plays (blocks)? Yes __, No __ |
| Question 5: | Do you restrict the time when the TV is on? Yes __, No __ |
| Question 6: | Does your child play video and computer games more than an hour/day? Yes __, No __ |
| Question 7: | Does your child have any vision related behaviours that worry you? Yes __, No __ |
Mild changes in visual processing functions may become noticeable when the demands in visual functioning increase. The child may not manage large groups of people, shopping malls or swimming halls if recognition of family members among many people is difficult. A child may not develop ability to finding ways between places that the child visits regularly. Social skills may not be at age level. These are some of the worries that parents or educational personnel may express.
When starting reading the child may see letters moving partially on top of each other; this is called crowding phenomenon and requires increased spacing between letters of words, maybe also lines.
Strabismus that occurs only for very short periods and causes double vision may make looking at pictures and texts unpleasant.
If a child has any kind of problems in using vision, a thorough examination is needed so that the problems can be solved well in time before the school starts. Occupational therapy should not be started before the visual functioning of the child is carefully assessed for all processing functions, after correction of refractive errors if needed so that vision can be correctly included in therapy.
Children with vision and other disorders can often be thoroughly assessed so that a Profile of Visual Functioning can be reported for school education. Therefore the health care centre and child’s school for next year expect useful information from the ophthalmologist for planning of local services at the kindergarten or school or a private day care if the child’s condition prevents integrated education.
In several countries there are currently projects on planning of paediatric vision care as a part of improving interaction and bonding in the families. These new observations should be included in the general follow-up of the development of infants and children. The referral services should be improved at the same time so that refractive corrections and functional assessments become a part of the examinations and early intervention is started without delay. Further training of health care personnel and ophthalmologists and paediatricians is needed to make the new responsibilities well-known.
This document was last modified on