The Profile of Visual Functioning
To collect all the information needed in the assessment of visual processing functions we should have good collaborative work with the families and medical, educational, therapeutic, psychological, and rehabilitation services. Every one of the caregivers and educators observes the child during her own work and writes down observations that can then be discussed in the rehabilitation team. This increases the knowledge on a child’s functioning and slowly leads to correct support for the development of the child.
In the enclosed list (Figure 16) there is only one line for devices. This is because the vision rehabilitation services have their detailed lists of the needs of these children. The following three students’ devices may give an idea on the work that is needed in creating them.
A. 
C.  D.
D.
Figure 15. A. The girl had lost function in the right arm and hand, in the right hemifield, convergence, accommodation, and vertical eye movements; visual acuity and contrast sensitivity were close to normal. Therefore she reads with a CCTV pushing the text up on the screen because the eyes do not move downwards.
B. The text that is upside down on the large screen was for a boy whose saccades from right to left were so much more regular than from left to right that visual acuity was five times better, improved from 0.01 to nearly 0.05. Saccades and fixation often improve when children start reading so also in this case and a year later the boy was able to read in both directions.
C. The 6-year-old boy with the head stick had been diagnosed so severely multidisabled that “his vision could not be tested”. However, his parents noticed that he had learned to read without anyone teaching him. He was very hypotonic, with poor head control, poor fixation and no accommodation so he received progressive spectacles and a head stick and could start writing faster than other children of his age. Because of hypotonia his head is gently supported during writing, which is a demanding static working position for the classroom assistant.
The long list of common problem areas helps remembering nearly all functions that should be observed and assessed (Figure 16). Part of this information should be received from the medical services. The functions that should always be reported by the ophthalmologist and optometrist are:
- ocular motor functions, of which fixation of penlight and small picture, saccades, accommodation, strabismus and binocularity are the most important
- refraction and correction with the spectacles, under- or overcorrections, and at what distances the child has the clearest images
- results of all clinical tests that were possible to use, name of test and distance used
- visual field as carefully as possible, size, structure of central field (if possible to describe and measure)
Visual acuity, contrast sensitivity, colour vision and observations on the use of central visual field are best performed at kindergarten and school, which is possible after teachers, therapists and parents are trained to observe and report visual functions. Teachers and therapists can learn to use more than twenty usual tests together with the school nurse and/or psychologist and need help in the interpretation of the findings and their use in planning special education. Development of collaboration between medical services, schools, early intervention specialists, and social services is central in the development of assessment and observation techniques and special education.
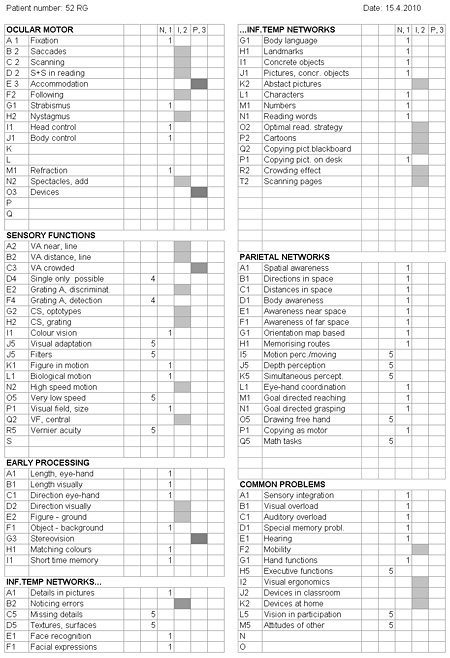
Figure 16. An example of the list of visual functions and vision related activities considered in assessment of educational needs. Functions and activities are marked as normal (N, 1), impaired but useful (I, 2) or profoundly impaired (P,3). They are characterized, for example “profoundly impaired accommodation” as E3, which is easy to move to the Excel when collecting the results for the summary of findings
The findings in the Figure 16 were recorded after the first clinical assessment of a 6-year-old boy. The Profile is a summary of observations at the kindergarten and at home, somewhat modified after the clinical examination. New spectacles would compensate for his weak accommodation and would improve all near vision tasks but will not remove the basic problem. The effect of a telescope and other devices on visual ergonomics would be experienced after training and would change the Profile.
If we mark in the list the quality of each function as either normal/typical to sighted children (=1), typical to children with impaired but useful vision (=2) or the child uses strategies typical of profoundly visually impaired and blind children (=3), we can at a glance see in how many areas functioning is normal or close to normal, restricted or barely possible. If a function is not assessed because of limited time, communication problems, or because the child was tired or lost interest, it is marked with number 4 and needs to be tested in near future. If the child has not had enough previous exposure to a similar task, as in the list above “Missing details”, it is marked with number 5 = “to be tested when possible” and the function will be tested during the next assessment after training in the kindergarten or school.
If we are reviewing findings in a cohort, we mark each functional area with its letter and number, for example: in Ocular Motor Functions, Accommodation – E3 is recorded in the Excel page “Ocular motor functions”. Other students’ findings in accommodation are recorded in the same column, after which the resulting numbers of different types of accommodation are calculated.
There is space for a few other functions on each Excel page for other less common functions in a cohort of children but rare individual functional losses and strengths need to be reported on a separate page.
It often takes more than two years to fill the profile but rather soon it is possible to answer the most important questions and mark the rest as functions that require further assessment. In areas of reading and mathematics especially but also in physics and chemistry, woodwork/sloyd, and home economics teachers have their own lists of questions for fine adjustment of teaching and learning strategies. Strategies can be trained also during visits at the resource centres if they are available.
At a glance one can usually see in the profile that there are more normal functions than impaired functions among the functions that could be assessed, as in the case in Figure 16 where only accommodation was severely affected. Loss of stereovision is rarely a problem in activities and tasks of children and they do not choose a work where stereovision would be important. The finding of many normal functions is especially important to the parents who often learn only about functions that are impaired.
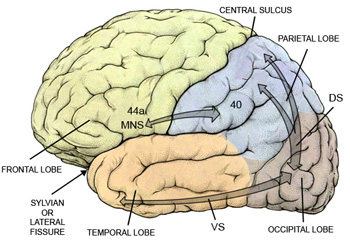
Figure 17. In the above picture we see the arrows depicting the flow of visual information as they usually are drawn toward the parietal lobe as the dorsal stream (DS) and toward the lower surface of the temporal lobe as the ventral stream (VS). However, as stated earlier, the top-down flow toward the occipital lobe is stronger than the flow toward the parietal and temporal lobe. The arrow from the anatomic area 40 to 44a shows the location of the third interesting network called the mirror neuron system in monkeys.
The mirror neuron system in monkeys. It was described in early 1990s (di Pellegrino19926) and contains visual and visuomotor cell groups (Sakata et al 19957) that are active during goal-directed movements, especially those of hands and mouth but also when monkeys watch someone performing similar goal-directed movements; i.e. they “mirror” motor functions. There are also cell groups that are active during the sound that the monkey has experienced during a movement even if the movement is hidden behind a screen, or during a movement toward an object that was visible before but was hidden behind a surface before the movement started. It is the Act/Goal-directed movement that activates specific cell groups. Findings related to mirror neuron networks are made in experiments on behaving monkeys but corresponding parts of the human brain are active during movements and observation of similar movements.
Activity related to emotions can be recorded in the area called Insula, which is located deep in the Sylvian or lateral sulcus and is not visible on the surface of the brain8. The monkey and human infants are able to copy facial expressions8 starting at the time of birth and follow facial expressions and goal-directed hand movements of adults and other infants and children long before they can perform similar hand movements. By observations of often-repeated activities infants learn to anticipate the goal of several activities before their first birthday. The brain structures that function in the human infant in the way typical to mirror neuron system of monkeys have not been confirmed but it is obvious that these functions are important in the early communication and interaction. Infants are extremely sensitive to the emotional status of their mothers9 and “diagnose” depressive behaviour of the mother better than medical experts. They distance themselves from the interaction turning their face away from the mother.
Visual functions that are likely to be connected to mirror neuron system are not in the profile in Figure 16, which is primarily thought for assessment of children at schools, the flow of information between schools and hospitals/private offices. The profile of visual functioning in infants and young children will contain many functions that are typical to “mirroring functions”. It requires still collaborative development in several early intervention teams to decide which functions should be assessed at which age. Often it is easiest to use the usual long list and mark with the number 5 the functions that cannot be assessed.
Damage to “mirror neuron system” has been suggested to be a cause of autism but this is difficult to prove. In all communication problems, however, we can support the development of interpretation of facial expressions by bringing the infant’s hands on the face of the adult person so that the infant experiences facial expressions through visual, tactile, kinaesthetic, and auditory information.
![]()
![]()
![]()
[ Instructions I Paediatric Vision Tests I Vision Tests ]
This document was last modified on