
Low Contrast Face Test for Communication Distances
#253500

At the age of 12 weeks at the latest, infants respond to a friendly smile with a happy “social smile”. Their mirror neuron system makes it possible to “mirror” facial expressions if the baby can see facial features clearly enough to copy them. Therefore, if an infant does not respond to smiling faces, eyes and vision need to be thoroughly examined. In this examination the Hiding Heidi test is important for testing whether there is a difficulty in perception of low contrast facial features at usual communication distances.
Visual communication is the most important way of communicating during the first year of life. Expressions on faces are mediated by faint shadows and changes of the contours of the mouth and eyes.
Hiding Heidi test is designed for assessment of low contrast information in communication situations in infants, children and adult persons who are unable to respond verbally or by pointing. If the infant/person can follow a moving target or shift gaze to or turn head to peripherally presented visual stimuli, preferential looking test situation can be used. A preferential looking test situation is a detection test and does usually not depict how the infant or child perceives the test picture. However, if an infant responds with a smile, he must have perceived the picture of a smiling face.
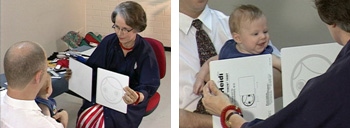
Figure 1. Hiding Heidi picture presented in a preferential looking test situation to an infant at the age of 3 months.
The test picture is exposed from behind the white card by moving the cards in opposite directions with the same speed. The normal reaction is that a young infant follows the picture of the face with a combined movement of the eyes and head (the differentiation of eye movements from head movements has not yet developed). If the infant follows the card and smiles like the 3-month-old infant does in the above picture, he must have perceived the smiling face and responds with an age appropriate social smile. In the brief moment of the test you have received information on the infant’s visual, motor and emotional development. The prerequisite for an age appropriate response is that the infant has a normally functioning mirror neuron system and can perceive facial features.
If an infant does not respond to smiling faces, eyes and vision need to be thoroughly examined. In this examination the Hiding Heidi test is important for testing whether there is a difficulty in perception of low contrast facial features at usual communication distances.
By presenting the test at different distances it is possible to assess how close the people should be in communication situation so that the infant can perceive faces. If an infant only responds to high contrast pictures of Heidi, the people in his or her life should be aware of this problem and make their faces more visible. This can be done by wearing lip and eye liners, bright lipstick and eyeglasses with dark frames. Men can use brown lip liner.
The question of “normal values of the Hiding Heidi test” is not a relevant question. We are not comparing the communication situation of a visually impaired infant with that of a normally sighted infant. We want to find the contrast level where the infant can perceive the face of a communicating person, with or without increased make-up.
Instructions
Before starting to test, notice how far the infant becomes interested in people around him and how often he looks at faces and at which distance. Hiding Heidi pictures are usually used to find the contrast level an infant needs in usual communication distances.
Position the infant so he or she faces the tester in an optimal position for participation in the test situation. If possible, select for the first functional assessment the time of day when the infant is most alert.
Start the test at a distance that is usual to the infant’s communication situation. Hide the full contrast stimulus card behind the blank card. Tap on the white card to guide the infant to look in the direction of the test and say something softly, e.g. “I hide a Heidi face”. Move the blank card off to one side and the card with the face picture off to the other side at the same speed. The card with the picture should be moved to the right or left in a random order. (If the infant seems to have fairly normal visual functions, you may shorten the test and start with the picture at 10% contrast.)
If an infant does not respond to a horizontal presentation of the face cards, try vertical presentation.
When you find the distance and direction of presentation that work, present the cards in the order of decreasing contrast: full contrast, 25%, 10%, 5%, 2.5% and 1.25%, each card once as long as the infant responds with a following movement.
If the infant does not follow the movement of the face picture at a low contrast level, place the picture behind the white card and say ”Heidi is hiding now”, tap on the white card and then present the picture again.
If you do not see the usual response, go to the previous contrast to confirm the threshold level. If the infant responds, you have found the threshold contrast for the present distance. If the infant does not respond, he has lost interest and you need to play with another test game and try again later.
To perceive facial expressions on young faces of the parents the infant needs to have both perception of low contrast information and motion perception. After a short play situation try the contrast level that did not work but now at a shorter distance from the child. Keep your voice soft and friendly.
If you get responses to the picture with 10% contrast at a distance of 40 cm (16 inches) but not to the lower contrast pictures, observe the infant’s communication with parents when they have increased contrast on their face. If more contrast improves interaction, add also tactile information in the early intervention, i.e., the little hands on the face of the parents. It gives the abstract visual information a more concrete content.
Inform all persons who are related to the child about the importance of the short communication distance and use of tactile and haptic information and voice to support visual information.
Recording the result:
The infant responded to the picture at 25% contrast at a distance of 60 cm (2 feet) and to the picture at 10% contrast at 40 cm (16 inches) but not to the pictures at lower contrast levels. Since the test was performed without near correction, it needs to be repeated when the infant has become accustomed to the use of the new spectacles. Increased make-up seemed to improve visual communication. Use of tactile information for supporting visual information was demonstrated and recommended.
If another 3-4-month-old infant follows the low contrast face pictures in the preferential-looking test situation until 2.5% picture at the usual communication distance but does not smile to the picture or people smiling to him, paediatric neurologist should assess brain functions carefully to answer why the brain does not use the available visual information in communication situation. At the same time early intervention should be started to build effective communication through observation of body language, tactile and auditory information and carrying the infant in a sling all day long so that he can experience movements, changes in positions, and bodily closeness.
An infant who does not experience bonding through vision needs to get confirmation of being loved and close to parents through all other senses more than a normally sighted infant.
Normal values of the Hiding Heidi test
The question of “normal values of the Hiding Heidi test” is not a relevant question. We are not comparing the communication situation of a visually impaired infant with that of a normally sighted infant. We want to find the contrast level and distance where the infant can perceive the face of a communicating person, with or without increased make-up.
The “normal values” would be difficult to measure because the sphere of visual interest and attention grow with varying speed in infants at the same age even if the cohort would be infants with typical development. Uncorrected refractive errors would affect the recognition of facial features. For such an investigation we would need to have pictures with many more sizes, if, for example, the measurements would be made at half the maximum distance of the visual sphere of each infant. So far there has not been a well-founded demand for this type of information.
[ Instructions I Paediatric Vision Tests I Vision Tests ]
This document was last modified on