2. Communication - interaction

In an infant and a young child, visual impairment often delays all areas of development if early intervention is not started early and the infant/child is not taught compensatory techniques. Among the areas of development that are the most important during the first year are:
- communication and interaction
- motor functions
- development of spatial concepts
- orientation in space, egocentric and allocentric
- development of object permanence and
- development of language
Later development of social skills and self image is related to how the peers and adult persons respond to the features caused by the visual impairement. Many visually impaired children and teenagers experience communication and interaction as their most limited functional areas that therefore should get special attention right from the start.

A newborn baby recognises significant adult persons and children by smell, voice and the way they hold him/her. At the age of a few weeks visual information starts to get a dominant role in interaction. Vision carries the information that tunes in the adult person and an infant as shown in this picture from Anne Nafstad's and Inger Rřdbroe's book 'Co-creating Communication' (Nord-Press, ISBN; 87-89109-60-0) between mother and infant.
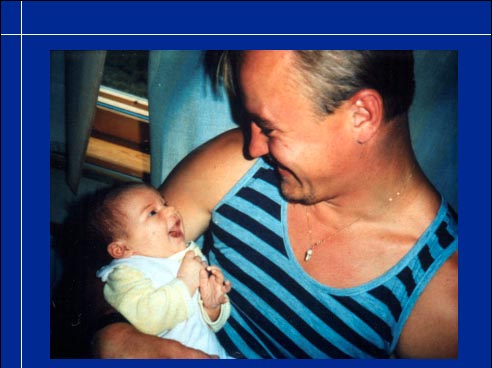
Visual communication is equally important between father and infant. They understand each other quite well and are able to convey the joy of interaction when a normally sighted infant is three months old.

Video
When an infant is visually impaired as this infant who has colobomas in both eyes, early interaction is affected by the irregular eye contact. Because the maculas are pulled upwards from their normal location, the infant seems to look above the hairline of the adult person when actually looking at the eyes of that person. In our western culture we expect 'normal eye contact' during communication and experience a deviation from this pattern as a sign of lack of interest. Even when one knows the cause of the 'abnormal' behaviour one has to remind oneself now and then of it to avoid negative reactions.
This infant was also functionally deaf at that time. Therefore communication was supported by tactile information, TADOMA, by holding the little hand on the lips or close to the vocal cords to give him an idea about spoken words.

Vision for communication needs to be assessed early. We can measure visual resolution with grating acuity tests and contrast sensitivity with the Hiding Heidi low contrast face pictures during the first 18 months and with optotype tests starting at the age of 20 months.

Video
Measurement of grating acuity and contrast sensitivity take little time when the infant has normal vision. During the measurement we also learn that the infant responds to the smiling Heidi face with a smile, which means that he not only sees the picture but can also copy the expression. When an infant is visually impaired, and especially if there are other functional problems, these measurements may take time. Sometimes the responses are different in different postures so several measurements may be needed before the capabilities and weaknesses in functions are assessed.

The Hiding Heidi pictures are printed at 100%, 25%, 10%, 5%, 2.5% and 1.2% contrast. The test is performed well within the visual sphere of the infant/child and depicts how low contrast visual information is perceived by the child. Our expressions are conveyed by faint shadows on our face, especially faint on very fair Nordic faces or on very dark faces.

When contrast sensitivity has been found to be low, contrast on the adults' faces needs to be enhanced by using contour pen, eye liner, spectacle frames etc and by holding the infant very close. Decrease in distance enlarges the image on the retina (geometric magnification). Tactile information can be used from very early age to support communication via visual and auditory channels.

In all cases of early visual impairment, measurement of refraction and accommodation should be a part of the primary investigation. The infant should get glasses if the refractive error is large enough or cannot be compensated by accommodation.

Video 1 & Video 2
The role of accommodation was very obvious in this neurologically otherwise normal infant who had just been diagnosed as having 'infantile autism' because she 'avoided eye contact', turned her head away when an adult person, even her mother, wanted to communicate with her. Usually, bringing hands to the midline helps the infant to bring also gaze to the midline but it did not help in this case. The refractive error of the infant was only +1.0 in both eyes and she did not show any accommodation when her eyes shortly looked at the high contrast targets next to my retinoscope. When +4.0 glasses were put in front of her eyes to give her a clear image on the retina without accommodation, there was a momentary change in the infant's behaviour: first surprise, then eye contact with the mother and then happy social smile for the first time.
I have been asked, why the glasses cause this kind of a response. I do not know. The infants do not remember this moment when they are old enough to talk and there is no way to measure what happens in the brain of the infant the moment he or she sees a clear image at near distance for the first time. Based on what we know about infant visual system today, the resolving power of the infant's visual system is not so good that +4.0 glasses should make a major change in the image quality. Yet it is obvious that the experience of clear image has great emotional and communicative value.

Video
This infant had had infantile spasms and therefore a treatment with ACTH and seizure medication. Because of medication and because of her abnormal brain activity she had a low level of wakefulness. During the first examination she did not wake up at all (video sequence 1). During the second examination she woke up but did not fixate her gaze on any of the visual targets used. Her state of accommodation did not change when objects were moved closer or farther away from her. When near correction lenses were put in front of her eyes it took a few seconds for her to become aware of the new kind of information before she responded with eye contact.
Infants with severe hypotonia and insufficient accommodation seem to later develop strabismus, which often is difficult to treat.
These two infants showed an immediate response to near correction. Multihandicapped infants and children may require repeated exposure to the clearer image to respond to it. Therefore the lenses need to be available on loan for observations at home and/or in the day care.

When we assess vision for communication we can measure grating acuity with the Teller acuity cards or the LEA GRATINGS and contrast sensitivity with Hiding Heidi pictures, which also often reveal an adequate emotional response to the smiling face picture. When the child is two year old or functionally at that level, we can measure visual acuity and contrast sensitivity with optotype tests. Measurement of refractive errors and accommodation are possible at the age of a few weeks and should be an integral part of all clinical examinations.
Observations on whether the infant recognises family members and other related people can be made toward the end of the first year. Perception of facial features can also be observed quite early if the tester approaches the infant without saying anything, just smiles to the infant. Response to the Heidi face is another early observation that is often possible at the age of eight to twelve weeks.
When the infant comes to a group of infants in day care, it is very important that the infant's visual communication with the other toddlers is observed. If the infant has difficulties in seeing visual communication, the play situation must be well structured and an adult person needs to function as an interpreter to facilitate communication between the visually impaired infant and the other toddlers.

Heidi Expressions pictures were designed to improve diagnostic work on vision for communication. There are six common expressions, two happy, two sad and two serious. The cards can be used to discuss different emotional states with a young child while searching for pairs of the cards.

There are two exactly similar cards of each expression and a third where Heidi has a bow. If a child does not see the difference in the expression of the mouth (s)he is likely to match two cards where Heidi has the bow as the similar ones. In such a case we can direct the child's attention to the form of the mouth and discuss what Heidi might express with her mouth in the (us) different pictures.

There are cards on 100%, 10% and 2.5% contrast to measure the effect of contrast on the visibility of facial expressions.

When a child does not seem to 'understand' the different expressions on the Heidi Expressions cards we need to observe the child in play situations to see whether expressions with colour and motion information are perceived by the infant. We can make visuotactile pictures. Visuotactile pictures are for example pictures, where on a paper plate two buttons represent eyes and a piece of pipe cleaner depicts the mouth. We can use them and mirrors to assess the difficulty in seeing expressions. Colour photographs and videos are often easier to understand than abstract pictures in black and white.
If after all these diagnostic play situations the child does not show any understanding of facial expressions (s)he needs an interpreter in communication situations. Even if the child may move freely without bumping and has normal visual functions in other areas of higher visual functions, vision for communication may be impaired or lacking. In these situations the child needs an interpreter in group communication situations. This is one of the most difficult interpretation tasks because toddlers do not understand the spoken language very well.

If recognition of family members and peers is difficult, the child needs to develop compensating techniques by learning to recognise people by their clothing and their voices.

In the assessment of vision for communication we presently have two problems that need to be solved in the future:
1. many ophthalmologists do not measure refraction of young multihandicapped infants during clinical examination even if the examination is done under anaesthesia and there thus would be good opportunity to measure the refractive error. If the therapists and teachers request for this information, the measurements will be done in most hospitals and private offices.

Similarly,
2. accommodation is not measured as a part of routine examinations although it takes very little time. However, plus glasses can be used by anybody to observe whether they improve vision for communication - as we saw in the two videos.

Also, everybody can observe early interaction and be aware of the possibility that lack of interest in early interaction may be caused by insufficient visual information for communication.

When ever an infant or child is thought to have autistic behaviours it is necessary to measure the functions that have been discussed in the previous slides: type of fixation, refractive errors, accommodation, oculomotor functions, recognition of facial features and perception of facial expressions. Quality of peripheral hearing and perception of spoken language are equally important functions to assess, especially if the child is found to be visually impaired.
In the assessment of school age children it is important to briefly discuss how they find their school and peers, do they have friends and how they experience their situation in the group of their peers. If there seems to be any problems in the acceptance of the impairment and/or in the communication/ interaction, a more thorough assessment of the child's situation is warranted because depression is not an uncommon finding in the pre-teens and teen-age years (for more information see Berit Lagerheim's article).