Assessment of Visual Functioning
of Disabled Infants and Children
as
Transdisciplinary Team Work
Slide 36.
I would like to stress the text in slide 36. Tests for measurement of visual functioning are easy and do not require much time and can thus be used by teachers, therapists and school nurse to assess the child’s functioning at school. During the projects at special schools in Finland we have learned that many test situations result in better values at school than in the hospital or a private office. The causes are: 1) the child does not need to wait, teachers choose the child who seems to be in the mood of being tested; 2) the presence of child’s own therapist supporting the child during measurements and his classroom teacher and assistant watching him, which improves motivation and concentration so that “a student with short concentration span” participates in the test situations for a full hour. When the classroom teacher and assistant can see the child’s behaviours during the tests they understand the test results better and also appreciate good ergonomics, which has immediately improved students’ classroom situation.
If the test results show major difference from the results in the hospital, they should be discussed with the ophthalmologist to improve the test situation in the hospital as much as possible. Usually it is not possible to arrange a comfortable test situation if the student comes to the hospital in his electric wheelchair, which cannot be placed close enough many instruments, especially perimeters. One possibility for good assessments of the difficult-to-test students would be to have parts of their medical assessment at the Schools for the Blind and Visually Impaired where the classroom teacher and assistant and the child’s therapist could be with the child.
Slide 37.
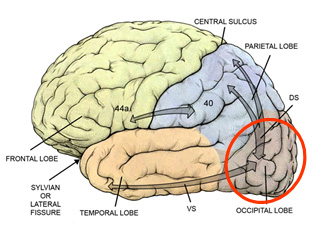
Visual processing functions are best assessed in the order where they occur, first the early visual processing in the occipital cortex, then the higher processing functions in the dorsal and ventral networks (“streams”) and in the mirror neuron system. The name “stream” would mean that there is flow in one stream. When you look at the arrows on the picture, you see that the arrows are thicker toward the occipital cortex than from it. This the typical feature of the functioning of the visual systems, the Top-Down flow defines which parts from the visual information flowing into the lateral geniculate nucleus (LGN) will be allowed to enter the brain.
Early visual processing includes coding of colours, contrast edges, movement/ motion, line directions and length, fusion of images and stereovision, perception of objects and figures on patterned background, visual closure, filling-in, and visual illusions. Although the cortical areas in the occipital lobe are called visual cortices we should remember that also short term memory, tactile, haptic, and auditory space are represented there and compete from the use of the same networks.
Slide 38.




Perception of direction of lines and objects is among the most common problems in children with CP. The LEA Mailbox test is a quick test for the use of directions in eye-hand coordination. Awareness and discrimination of directions of lines as purely visual recognition task can be studied with several picture series of angles of different sizes and educational toys where lines are moved to become parallel. Having the concept parallel and ability to compare the size of angles and geometric forms are functions that can be observed in kindergarten play situations. Similarly length of lines and objects is a function in early visual perception.
The LEA Rectangles test game is also a test that a 3-year-old child performs as a play (Slide 38). Of the many educational games Colorama requires simultaneous use of both colour and form comparison. These three games show good use of basic components of pictures in the test situations in Slide 38. However, on the next higher level in the ventral networks/stream area this child does not understand what is meant with mouth in simple pictures of faces because she has never looked at faces, she has prosopagnosia, face blindness.
There are several other tests for the assessment of early visual processing functions: fusion and stereovision tests can be used in the assessment of children who have binocular vision and have developed binocularity. These two test situations are usually not used by psychologists although for functioning at school it is important to know whether the student has stable or weak binocularity or has alternating strabismus, which often requires reading lens for the eye preferred for reading and distance correction for the other eye to stop the constant hopping between the alternating eyes.
Slides 39 and 40.
The preschool assessments are completed covering all the questions that have been asked in the Kindergarten and questions that the teacher(s) at the school have asked during and after the planning meeting, leading to the first Profile of Visual Functioning for School.
Slide 41.
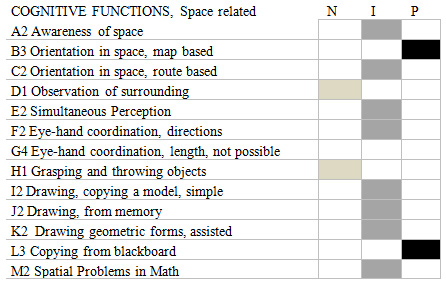
Profile of Visual Functioning for School
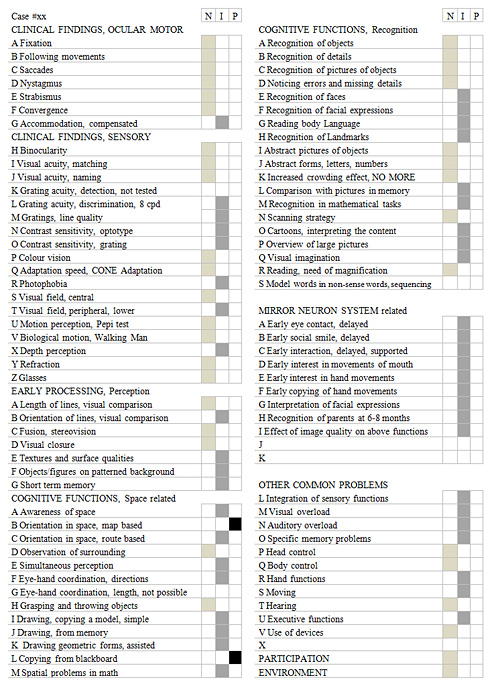
For the Table in slide 41, teachers, therapists and the family had marked their observations that they wanted to either confirmed or corrected. After assessments at the low vision clinic and at the school, the child’s visual functioning in each of the functional areas was marked as either normal (N), impaired (I), or profoundly impaired (P). If vision’s role in a function is felt to be normal, then the child is supported in learning and taught like a normally sighted child. If vision is felt to be atypically used, the use is tested and observed further to find a strategy that best fits the child’s needs, sometimes even techniques typical to blind children are used in teaching these “sighted blind children”, normally sighted in many functions, impaired in some and using strategies typical to blind children in a few functions. In functions where vision is profoundly impaired, the strategies typical to blind children are considered, auditory and tactile learning materials and training of speech and language related memory. In each case the effect of other common problems is considered. This is especially difficult task if the child has severe motor problems that require individual solutions in visual ergonomics and assistant’s involvement in tasks requiring eye-hand coordination.
Often eye-hand coordination cannot be assessed at all because the hands do not function. Some children can use their feet for writing and many other tasks. In the above list there are some empty spaces because those functions/tasks are usually not yet present at this age.
In many tasks several functions are required; for example, in moving in an environment that we know we are usually aware of where we are, in which direction and how far certain places are (called map based orientation). We use some landmarks to confirm that we are moving in the correct direction. Some children do not have map based orientation but must learn to remember the order of landmarks and move from landmark to landmark along a route. If something unusual happens on the road and the child turns to look at it, he may lose the track(?) because he is facing a landmark on its “wrong” side. Problems with directions are common both in the environment and as directions of lines in pictures and orientation of objects. Development of concept of directions we can observe already when infant start to play with puzzles. First they try to push the puzzle pieces in their places with force and then learn to turn them to find out whether they fit in the cut-out.
Slide 42.
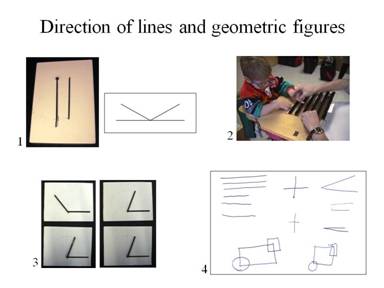
The awareness of directions of lines is an important function at school. Therefore varying test situations have been created to reveal in which situations directions of lines is difficult to perceive. In slide 42 there are some tests that are easy to use at school: 1) A thin metal rod is fixed on a piece of wood at both ends and another rod only at one end so that it can be turned non-parallel to the fixed rod and the child turns it until it is parallel, or the tester turns it guided by the child; similar visual task without eye-hand coordination is a drawing to ask an older child to describe in which directions the lines are; the student may answer that the lines move and it is difficult to know what the directions are. 2) Early training of direction using Velcro lines and “driving” with the finger or with miniature cars “in this direction and opposite direction”. When the child seems to understand that driving along the lines is the task, the transparent piece of plastic is turned so that the tactile lines are under the surface and at the same time the orientation of the lines is changed 90 degrees. If the child is now asked to drive along the lines, it is possible that the movement continues in the same direction as before, the 2 cm visible lines may not carry the information on direction because it is in the motor memory and related to tactile information, not vision. 3) Two angles with one side fixed on the surface and the other movable so that the tester can change it to make the angle different from the model angle (the upper angle on the left) and ask the child to say how much it needs to be turned so that the angles are again alike; 4) Drawing different basic forms with the child reveals varying difficulties in perception of parallel lines, angles and complex geometric figures. This student copied three parallel lines and the cross well considering the limited hand functions but copying the angle was not possible; he drew a line, then the pencil moved wiggling a short distance and after that he drew a line nearly parallel to the first line and said “I don’t know how you made the lines to meet. When it was told him that the second line is drawn from the point where the first line ends, he used this spoken information to draw a very small angle. He did not perceive the difference between the angles. He copied the forms “circle” and “square” on the two corners of the rectangle as he had seen them drawn by the tester. However, a student may copy forms that partially lie on top of each other as individual short lines, which reveals that he does not perceive the geometric form as we see it but uses the drawing as sequential information. (This slide was not shown during the lecture in Montreal but during the discussions the next day. It is, however, such an important part of the testing at school that it is included in this summary text. These basic concepts and several other basic concepts should be tested before they are used in teaching.)
Teachers and therapists need to know whether vision is the cause of an unusual way of using a function or several functions. Is there anything in the clinical findings of the ophthalmologist, neurologist, optometrist or orthoptist that could explain the behaviors? Therefore these long lists of observations on normal and atypical functions should be known during clinical examinations.
Mirror neuron system was discussed earlier and its main activity areas are included in the Profile: early communication and interaction, interpretation of emotions and intentions, and observation and copying of movements, especially goal-directed hand movements. All these functions can be disturbed if either motion perception or perception and recognition of visual information at low contrast levels is deficient. Therefore the clinical measurements are important.
Other common problems are not vision related but may affect the use of vision, especially motor functions and ergonomics, two functional areas that are often only partially concerned in the individual learning plans (ILP) and educational teaching plans (IEP). We should more often ask whether it is necessary that children sit during learning, especially if head and body control are conscious and require nearly all capacity for motor control. These same questions are in the profiles of other functional areas that should be available when we assess vision. One of the difficult questions in integrated education is noise, especially visual noise in the peripheral visual field due to numerous drawings, maps and decorations in the classroom, movement of other students and classroom assistants and auditory noise that may cause dizziness, balance problems, even epileptic seizures. All students would benefit from cleaning the walls of the front part of the classroom by moving the visual materials behind the students (if the teacher can tolerate it) and restricting auditory noise. Children should study in calm, least restricting environment.
When these findings at school are discussed with medical rehabilitation team and combined with the new clinical findings and new educational assessment, a few findings of the school’s educational team may change, for example reading may be planned using new reading strategies, devices and auditory and e-books. The Profile changes at least once a year, most often toward better functioning but in progressive diseases toward more demanding supportive strategies and devices, maybe a move for a short or longer period in the Resource Centre of the Special School for training of techniques typical to blind children.
Slide 43.
If normal functions (N) are marked with number 1, impaired functions (I) with number 2, profoundly impaired functions (P) with number 3, and functions that could not be assessed with number 4, the findings are easy to move to Excel tables for comparison within a cohort.
Slide 44.

The assessment of visually impaired infants and children, especially if a child has brain damage related changes in visual functions requires a large transdisciplinary team. In the above list there are only the more usually participating people. In complex cases the number of people involved often grows so big that we have to watch that rehabilitation does not become an additional problem in the family’s life. Sometimes when the clinical findings do not explain the functioning of the child we may have the opportunity to use laboratories of basic science. New instruments are available and many of them add new knowledge to the assessment of functions, the latest surprises being related to the variation in the type of saccades when observed using the new eye-movement recording systems. Video documentation during the assessments and all activities of these children record many details that we do not see during the assessment or play because we are engaged in the communication or preparing for the next activity. Videos are sometimes a cruel but at the same time an effective way for learning about one’s errors or poor communication during testing or teaching.
Although the planning and execution of the assessment of visual functioning as a transdisciplinary team is important we should not forget:
Slide 45.
Opinions of the students
Slide 46.
Participation
Slide 47.
Effect of the Environment
It is revealing to hear that the preferred environment is that in the Resource Centre where they experience themselves understood and where they are among children with different kinds of atypical vision with similar experiences in their local schools.
Slide 48.
I closed (?) the lecture with this picture of a puzzle completed by a child with CP and brain damage related vision loss. It reminds me of the life and functioning of visually impaired children. Many details are not in their usual places yet the children function amazingly well in their individual ways.
In many countries there are on-going projects to facilitate communication between all stakeholders and create routines that would ensure early detection, treatment and intervention of developmental problems. Hearing screening at birth is mandatory in Western countries, motor problems are assessed soon after birth and baby massage and physiotherapy are routinely started immediately after the diagnosis. Many eye problems can also be detected early; treatment of congenital cataracts, glaucoma, and tumors is started without delay but problems in visual development may remain undetected and without early intervention for months because we “wait and see”. These delays in diagnosis, treatment, and early intervention cause difficulties in visual communication and interaction and thus negatively affect bonding between the baby and his/her parents and early learning and may have a lasting effect on the quality of life of the child and the family.
Early intervention should start early when the vision problems are noticed, at or soon after birth. When the loss of vision occurs later in childhood, again early intervention should be a part of the first investigations and treatments. If we work as a transdisciplinary team we can take care of the many problems related to the visual functioning of infants and children and support their families.
References:
1.Hyvärinen J, Hyvärinen L, Färkkilä M, Carlson S and Leinonen L. Modifications of visual functions of the parietal lobe at early age in the monkey (1978) Med Biol 56:103-109.
2.Hyvärinen J, Carlson S and Hyvärinen L. Early visual deprivation alters modality of neuronal responses in area 19 of monkey cortex (1981) Neurosci Lett 26:239-243.
3.Hyvärinen J, Hyvärinen L and Carlson S. Effect of binocular deprivation on parietal association cortex in young monkeys (1981) Doc Ophtalmol Proc Ser 30:177-185.