Assessment of Vision in Infants and Children
for Early Intervention and EducationAssessment of vision occurs several times during childhood. Since there are so many different types of visual impairment this paper covers only some important features of assessment of the different groups of infants and children with impaired vision. I would like to stress three features in the assessment:
-
It covers all visual functions, form perception, colour perception and motion perception; not only visual acuity and the size of visual field.
-
Its goal is a thorough evaluation of strengths and weaknesses in all functional areas so that special education and early intervention can be tailored to meet the needs of each child.
- It is performed as a transdisciplinary activity.
In the assessment of infants, preschool and school children we can define four main functional areas where vision usually plays an important role (Hyvärinen 1985):
- communication, both person-to-person, group communication and distance communication
- orientation and mobility
- activities and tasks of every day life (ADL)
- sustained near vision tasks, like reading and writing.
In the assessment of infants and young children each of these functional areas gets an additional feature: the role of vision in the rapid development of each function, both at present and in learning the next level of functioning
Assessment of young infants
In the early interaction, vision plays a central role in communication. A normally sighted infant expresses the joy she or he feels in communication; we understand the infant without any explanations (Figure 1.A). A visually impaired infant may not see enough to copy the smiles of the adult persons and therefore needs enforcement through tactile and auditory information (Figure 1.B). Since the visually impaired infant often has to concentrate on listening and does not have the usual eye contact, the infant is in danger to be experienced as uninterested in interaction.
The most important task in the assessment of infants is to find out how much vision there is for visual communication, whether
- the infant uses central vision and thus has a possibility to have normal eye-contact or
- uses an extrafoveal area of the retina to look straight ahead and seems to look past when looking at a persons face
- how close an adult needs to be to be seen by the infant.


Figure 1. Early interaction of a normally sighted and a visually impaired infant. A. Visual communication of a normally sighted infant is an effective bonding function; the infant and the adult person understand each other right from the start. B. A visually impaired infant may seem to look away from the adult and needs tactile confirmation of the auditory communication when lip movements cannot be seen. In such a situation the parents and caretakers need support and training in early interaction. (Pictures are from video recordings in the “LH-Materials”.)
Our expectations on the infant’s responses are based on interaction with normally sighted infants and therefore it is difficult to accept and understand another type of response as a normal response in case of visual impairment. The communication situation needs to be explained to the adult persons several times. Video recordings of early interaction are effective in demonstrating the adult persons that the infant wants to communicate and enjoys interaction.
If an infant has hypotonic accommodation or hyperopia, farsightedness, that disturb communication, proper near correction lenses must be prescribed as soon as the difficulty in interaction becomes diagnosed, usually at the age of one to three months. If hyperopia is high, 6 dioptres or more, glasses are prescribed even earlier. A practical difficulty at that age is to find good spectacle frames that fit the small face.
Infants usually copy facial expressions quite early and respond in a meaningful way to many expressions. If these responses are not present, either the infant does not see the expressions clearly enough (anterior visual impairment) or the cortical analytic functions (mirror neuron system) or connections to memory have not developed. Toward the end of the first year it is possible to observe whether an infant recognises family members and responds to them differently from other persons. If an infant seems to have problems in recognition of facial features and/or expressions, specific communicative therapy is necessary to help the infant develop participation in social interactions.
Eye-hand-cooperation can be assessed from the age of a few weeks when the infant first hits objects hanging within reach and then starts to reach for and to grasp them. Visually impaired infants use mouthing of objects later than normally sighted infants because the tongue and the lips give more exact information about details than the blurred visual image. Visuotactile materials are important in helping the infant to combine visual information with tactile and haptic information. Many house hold items have interesting form, weight, and surface qualities but also different balls and special playthings can be available on loan.



Figure 2. In the pictures above a visually impaired infant, who had not yet found his hands, is placed on a visuotactile picture on a lightbox. When feeling it with his fingers, the infant became aware of his hands, watched them carefully and then brought them to his mouth to have more concrete information about this “new” part of his body.
Vision for motor development is the second most important aspect of the assessment. Reaching for objects and grasping, crawling toward an interesting toy and pulling oneself up to stand are all closely related to development of spatial concepts of one’s own body and of the surrounding environment. Therefore vision for development of spatial concepts needs to be assessed. Lack of detailed information on the near space is compensated by using playthings that give both visual, tactile and auditory information (Hyvärinen 1998). Visually impaired infants often have also motor impairments and thus get early motor training. Even infants without primary motor problems need guidance by an experienced therapist to avoid delays in their motor development. If the therapist has not previously taken care of visually impaired infants (s)he should get information and support from the early intervention team. The therapist is usually the person who works most closely with an infant and the family and learns to make important observations on the child’s use of vision and changes in it.
Infants learn motor functions by carefully watching and then copying movements of other children and adults, especially goal related reaching with hands and lip movements. They enjoy the play near other infants, which is clearly seen in the “Colour Bath” play groups where infants paint with edible colours mixed with yogurt (milk or soya milk based).


Also visually impaired infants with some sight enjoy this play situation, both watching other infants and creating colourful forms with their hands. Infants’ parents enjoy these play situations nearly as much as the infants.
During the first year, the number of tests for assessment is limited. At the beginning of an assessment we usually first evaluate motor functions, fixation, tracking movements, convergence and saccades, then binocularity by observing whether the eyes are looking at the same point in space (Hirshberg’s test, cover test and Lang stereo test), visual field with confrontation tests (Sheridan balls, Flicker Wand) and using rolling balls, visual acuity with grating tests and contrast sensitivity with Hiding Heidi test.
Visual anticipation and the infant’s ability to evaluate velocity can be assessed with the simple “castle” game where an interesting object moving at a certain speed is shown to the infant, then it moves with the same speed behind a 10cm “tower”, becomes visible between the first and the second tower, disappears again and reappears between the second and the third tower. If the infant can correctly analyse the speed of the object and its direction of movement, the eyes move with correct speed to look at the object when it reappears.
During the evaluation one needs to constantly keep in mind that responses may be affected by either changes in the image quality or irregular visual associative functions or both. By using test materials of different sizes, colours and contrast, the role of the peripheral, eye related changes in image quality can be assessed. Assessment of higher visual functions requires repeated observations of family members, therapists and early intervention specialists supported by the findings from the clinical examinations.
Assessment of toddlers
As soon as the child develops the concepts ‘similar’ and ‘different’ they can be used to train visual acuity tests. The test forms in the LEA 3-D Puzzle can first be matched with their cut-outs based on their colours, then on their black &white three dimensional forms, then comparing the forms and pictures of the same size and finally comparing either the puzzle pieces or the large pictures on the key card to smaller and smaller test pictures. When testing is possible using the high contrast pictures, low contrast pictures of the same test symbols can be used to measure form perception at lower contrast levels.
Binocularity tests become possible at the age of two years and stereotests like the TNO slightly later. At this age, visual adaptation to lower light levels often becomes delayed in retinitis pigmentosa and can be tested with the CONE Adaptation test as the first sign of abnormal retinal function.
Children with suspected brain damage related visual impairment need a thorough evaluation because it is possible to measure crowding phenomenon and observe the child’s ability to perceive directions of lines and eye-hand-coordination. Observation lists developed in Scotland by Gordon Dutton and in Nordic countries by Lena Jacobson and me should be discussed with parents and day care personnel to learn about difficulties in the use of visual information. It is of utmost importance that communication difficulties are diagnosed and treated early so that the child can develop communication skills using compensatory techniques if in group communication (s)he is functionally blind. Too many of these children who do not recognise faces or expressions are diagnosed as autistic based on their failure to function in a group of children. Likewise it is important to understand the child’s difficulties in spatial orientation or lack of perception of objects that stand still or those in motion. The observation list can be like the following:
Typical behaviours of children with problems in cognitive vision:
- Variation of visual functioning is the most common feature
- early development of speech as compensatory function
- the child prefers talking with an adult to playing in a group of children
- the child dislikes crowded places, clings there to the parents;
beaches and swimming halls are worst if recognition of faces isdifficult - the child starts drawing and painting late
- colours are used for coding more than by normally sighted children
- little interest in TV and comic series
- the child may show signs of spatial interpretation problems, stops at thresholds and shadows
- the child may learn letters and numbers early but does not learn to read except short words
- the child may become angry when someone moves her/his playthings or clothes even minimally.
A child may have one or several of these behaviours. These children also develop typical compensatory functions:
- effective use of memory as compensatory function
- the child learns to use siblings and adult persons as helpers when there is a demanding visual task, often in a very diplomatic way.
Since asking help is not allowed in many schools, visual tasks become frustrating and a child who was looking forward to going to school, becomes unhappy and may develop unwanted behaviours.
This same list of behaviours can be used through all preschool years. Milder difficulties in different visual perceptive functions become visible when the child grows and the demands on the different skills become greater. Since the number of children with brain damage related visual impairment is steadily growing proper diagnostic skills need to be created for early diagnosis and intervention. Children with problems in motor development, children with intellectual disabilities and children who were born as small premature babies are groups that should be examined and observed particularly carefully. However, cognitive visual impairment may be present in children with no other problems in their development and may affect only one single perceptive function.
Assessment of school children
In many countries visually impaired children are in local mainstream schools where there is little knowledge about special learning techniques and how to teach them. Therefore the visual functions of the child should be described so clearly that they can be understood by the classroom teacher and the teacher’s aid. It would be of great help if the functional assessment would be made by the itinerant teacher during her/his visit at the local school. Most of the tests can be used after rather short period of training. Interpretation is sometimes difficult and requires analysis of the video made during the assessment by the diagnostic team responsible for the services.
During the assessment one needs to remember that responses may be affected by changes at three different levels of the visual system (Figure 3.): 1. in the eye and/or the anterior visual pathway, 2. in the pathway between lateral geniculate nucleus and/or the primary visual cortex and 3. in the cortical or subcortical brain functions. Disorders of the anterior pathway affect the quality of the visual image, those in the posterior pathway cause visual field defects and increased crowding but may not damage the tectal pathway, which then transfers information to cortical functions bypassing the primary visual cortex. Disorders in the visual associative cortices are often patchy affecting specific small parts of visual functions.
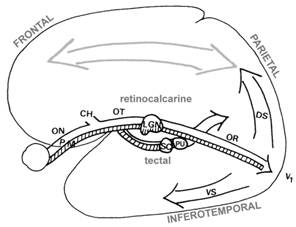

Figure 3. Visual pathways have two major routes, the retinocalcarine pathway via the lateral geniculate nucleus (LGN) to the primary visual cortex and the tectal pathway via the superior colliculus (SC) and the pulvinar (PU) to the associative cortices bypassing form analysis. Visual pathways transfer information through different neural pathways. The largest (approximately 80% of the nerve fibres in the optic nerve) is the parvocellular pathway (P) that transfers all colour information and high contrast black and white information. Its nerve fibres are thin and transfer information relatively slowly. The magnocellular pathway (M) comprises approximately 10% of the fibres in the optic nerve and transfers all motion related information and low contrast black and white information. Its fibres are thick and have high speed of information transfer. From the primary visual cortex information flows into other visual cortices in the occipital lobe (the early visual processing) and then three main directions, toward the parietal lobe’s dorsal networks (dorsal stream, DS ), toward the temporal lobe’s lower part as the ventral networks (ventral stream, VS ) and mirror neuron networks (MNS, mirror neuron system). Note that the arrows depicting the flow of information have two ends and the flow toward the occipital lobe, Top-Down, is greater than toward the higher visual functions that “demand” information from the lower levels. There are effective feed-back loops at all levels of the pathways; the visual pathways are ‘two way streets’. Connections between the different specific analytic areas are efficient and thus in a miraculous way the different components of the picture are combined to a clear, stable image although the components travelled with varying speeds through pathways of unequal length.
Before the functional assessment we need to collect all available information from the clinical examinations and laboratory tests. These are summarized by the ophthalmologist and the neurologist with special attention on findings in each of the three parts of the visual pathways. In some hospitals the clinical examination contains most of the measurements required for functional assessment:
- visual acuity at distance with a single symbol test and with a line test,
- visual acuity at near with single, line and more tightly crowded test
- contrast sensitivity with a low contrast visual acuity test, possibly also with a grating test
- colour vision with a quantitative test
- visual field with confrontation, with Goldman perimetry and as the reading field
- visual adaptation to lower luminance levels.
These measurements are repeated at the school (except Goldman perimetry) to find out variation in the measured values in different environments. Refractive errors and glasses are also reported by the ophthalmologist and the optometrist as well as all visual devices prescribed by them.
Disorders of higher visual functions may not have been assessed before or were assessed more than a year ago, so the list of the typical behaviours is discussed with the parents and the day care personnel. Mild losses of function may not be detected before school age if the child has been in a small group of children with well structured activities. Some children have developed effective compensatory strategies using siblings and adult persons as helpers in problematic situations. Specific problems in mathematics, reading and writing are often noticed first at school. The cognitive vision tests including observations on motion perception and spatial awareness complete the functional assessment.
What should the (classroom) teacher know about the child’s visual functions?
- Motor functions:
- fixation, is it stable, too short or not present; nystagmus with/without null position; is fixation central or eccentric
- are the saccadic movements accurate; compensated with head movements
- how regular are the tracking movements; compensated with head movements
- any involuntary eye movements during spasms or epileptic activity
- Sensory functions:
- visual acuity, all 4-5 measures with optotypes; smallest and optimal text size
- contrast sensitivity, at least visual acuity at 2.5% contrast
- colour vision,, confusion areas, which colours need to be avoided
- visual field for orientation and for reading
- visual adaptation, speed of adaptation, any effect on walking to school in twilight; can the child go out during breaks on sunny days when using his absorptive lenses
- Cognitive vision:
- does the child recognise people by their facial features, if not which compensatory techniques have been used for recognition
- does the child see expressions
- motion perception; does the child see objects that stand still as well as those moving
- does the child perceive size, length or does (s)he need haptic confirmation
- does the child see directions of lines
- does the child see details in pictures with many details
- eye-hand coordination, use of pencil and pen, drawing
- Prognosis: stable or progressive condition
- Vision for orientation and mobility, what needs to be considered in physical training
- What kind of vision the child has for sustained near work? Glasses, devices. Motivation and skills to use them; new devices to be considered during the term.
- Illumination at the desk and the black board, in the classroom and the corridors.
- Which devices should the school purchase, which come from other sources.
- Does the child have symmetric, normal hearing? Any other functional difficulties, disorders or diseases that might affect functioning at school?
This information is given to the classroom teacher and the child’s assistant and discussed again after a few weeks when the child has become accustomed to the new school situation. When the tests are made at the school in the presence of the teacher and the assistant they understand the test results much better than if they were only described in a report.
Since the tests can be used by all personnel categories, the assessment becomes a transdisciplinary activity. In the beginning it often requires assurance by the ophthalmologist or by the psychologist because it is quite deep rooted a belief that only doctors or psychologists may use vision tests. Child’s teacher and assistant need the information more than anyone else and thus are usually motivated to perform the repeated assessments during the term, especially visual functioning related to reading.
Written for this homepage 06.10.2002
This document was last modified on