Disorders of the Eyes and Anterior Visual Pathways
The changes in the quality of visual information can occur in all parts of the eye: the cornea may have unusual form or be cloudy, the lens and vitreous may be cloudy, retinal functions may be affected due to degenerations, diseases or trauma.
Changes in the structures of the eye may affect vision leading to:
- distortion and/or blurring of the image,
- decrease in visual acuity and/or grating acuity,
- contrast sensitivity,
- colour vision,
- adaptation to lower luminance levels,
- photophobia,
- visual field loss,
- loss of binocularity,
- loss of motion perception (rarely), which can sometimes be seen in diffuse retinal degenerations like retinitis pigmentosa.
A 3-dimensional model eye is useful when explaining the place of damage to the children and their parents as well as all persons involved in the care and teaching of the child. It is also important to be able to draw the basic structures of the visual pathways (Figure 4.B) while talking about them. This because most people have no information about vision except that it is the most important avenue of information and that vision is the image in the back of the brain. Show on the drawing where the damage is located if it is known. After this brief information many families and workers want to learn much more.
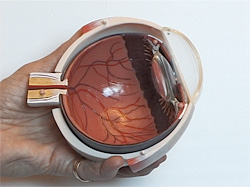
Figure 1. A 3-dimensional model eye is helpful in explaining the changes in the different layers of the eye. Changes in the quality of visual information can occur in all parts of the eye: the cornea may have unusual form or be cloudy, the lens and vitreous may be cloudy, retinal functions may be affected due to degenerations, trauma or diseases (in children retinopathy of prematurity is still a common cause, now fortunately decreasing).
In rehabilitation and education it is crucial that the child and his family as well as therapists and teachers know 1) the child’s condition, 2) what the different measured values mean and 3) what functions should be trained and supported in near future. During the diagnostic work-up at the hospital there is often tendency to describe the parents all the functions that are deviant from norm and pay little attention to the strengths of the child. In rehabilitation and education we build on the strengths of the child and therefore the profile of visual functioning is a useful tool.
To understand the visual functions some basic facts should be known about the structure of visual pathways as well as about the complex processing functions.
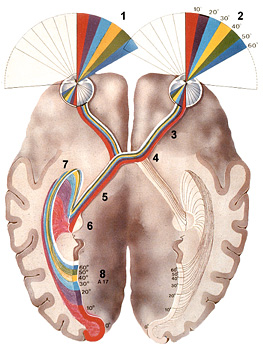
Figure 2. Parts of the visual pathways: retinas collect the optical information in temporal and nasal parts of the retinas from the opposite part of the visual field (1,2); the information is transferred through the optic nerve (3), optic chiasm (4), optic tract (5) to the lateral geniculate nucleus (LGN) (6), where the information undergoes major changes. From the LGN the optic tract (7) brings the information to the primary visual cortex (8).
Changes in the quality of visual information can occur also in the retinocalcarine pathway from the retina to the lateral geniculate nucleus. Atrophy of the optic nerve is common in children with brain damage. It causes loss of functions in the central visual field leading to relative central scotomas of varying size and thus a decrease of visual acuity, contrast sensitivity and colour vision and may also cause photophobia. Damage in the area of optic tracts or optic radiations causes losses in the visual half field on the opposite side (hemianopia).
The main pathways from the eye to the brain cortex are the retinocalcarine pathway via the lateral geniculate nucleus and the tectal pathway. The optic nerve and pathways have several different types of nerve fibres. In the retinocalcarine pathway the parvocellular fibres (P) (80% of all fibres) dominate. They are thin and therefore the speed of the movement of the visual information is slow. These fibres transfer colour and high contrast black and white information. The second largest group of nerve fibres are the magnocellular fibres (M) (10%).
The difference in the function of the two main neuron populations of the visual pathways can be roughly demonstrated by the following two pictures in Figure 3: If you keep looking at the STOP sign in the lower left corner of the Figure 3.A, after a while the grey dot in the upper right corner fades away (if you can resist the temptation to look at it) but the flickering grey dot in the Figure 3.B does not disappear even if you keep your fixation steadily on the STOP sign and also the non-flickering dot is visible now and then.
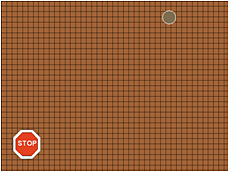
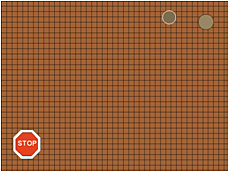
Figure 3. Cover the right picture when you watch the left picture and vice versa. A. If you keep your fixation steadily on the STOP sign, the grey dot in the upper right corner fades out. B. Even if you keep your fixation steadily on the STOP sign the flickering dot does not disappear and helps the non-flickering dot to become visible now and then (mostly because you cannot resist of briefly looking at the flickering dot).
The magnocellular fibres are effective in the transfer of low contrast black and white information and information related to motion/movement. They dominate in the tectal pathway that leaves the optic tract before the lateral geniculate nucleus (LGN) and transfers information to superior colliculus and pulvinar and many other cell groups that have specific functions. This fast pathway remains functioning if a child has large damage in the occipital lobes. Description of the tectal pathway helps the parents to understand why their blind child can move without bumping in obstacles although no recognition functions can be measured. Visual functions in the middle of the brain are coarse but fast and often save our life by warning about something possibly dangerous moving and we react avoiding it before we have seen what that “something” might be.
A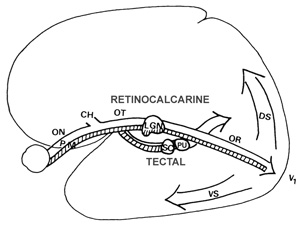
B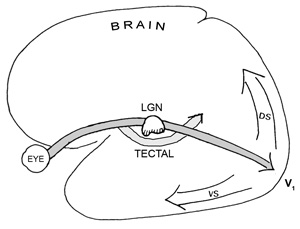
Figure 4. A. The pathways from the eye to the cortex have two main components, the retinocalcarine pathway over the lateral geniculate nucleus and the tectal pathway, which leaves the optic tract (OT) and transfers visual information to superior colliculus (SC), pulvinar (PU) and many other specific cell groups. From the primary visual cortex (V1, V2) the information moves to other visual cortices and then to ventral (VS) and dorsal (DS) streams/networks. B. A simple drawing for explaining the pathways to families.
![]()
![]()
![]()
[ Instructions I Paediatric Vision Tests I Vision Tests ]
This document was last modified on