Clinical Evaluation of Colour Vision
When a person's colour perception is deviant from that of the general population, the disorder may be either a congenital or an acquired colour vision defect.
Congenital Colour Vision Defects
Colour vision testing is designed for assessing children and adults who have congenital colour vision deficiencies. Often, the deviations from normal colour vision are so mild that they do not have any practical consequences, especially in childhood if the teachers and parents understand the child’s difficulty. Adults with colour vision defects should also be aware of this characteristic in their vision because some jobs require good, or even perfect, colour vision.
In congenital colour vision defects, the abnormality is usually in the structure and function of a cone pigment (rarely in more than one). Red-green colour vision defects are X-chromosomally inherited, thus more common in males (8%) than in females (0.4%).
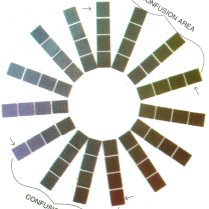
A normally sighted person sees all colours of the spectrum (Figure 2A) whereas a person with a red-green defect (Figure 2B) has a grayish confusion area (In brackets in Figure 2B) within which he or she does not see the difference between some shades of red and green and misses them.
 |
|
|
| Figure 2A | Figure 2B |
Figure 2.
A. Coloured surfaces in this figure represent all spectral colours, saturated at the outer end of the spokes.
B. This illustration depicts how the picture in Figure 2A is seen by a person with a deutan defect. Green tones and the opponent tones of purple-red are seen as dull and therefore easily confused with each other. Since these colours are on the opposite sides of the colour circle, there is an "axis" of deficiency across the colour circle. The colour space of this person is blue-yellow with confusion of colours in the red-green axis. Individual variations in confusions of hue are great.
(Figure 2 is reproduced with permission from Anders Hedin, MD.)
Colour vision defects are generally screened using pseudoisochromatic Ishihara-type tests. They are designed to be highly sensitive and usually miss only a few mild cases. Some individuals who do not have a colour vision defect may fail colour vision screening tests. Therefore, the degree of colour vision deficiency should be evaluated using quantitative tests. Statements or diagnosis of colour deficiency should never be based on screening tests alone. Widely used sorting tests of the Farnsworth Panel D-15 type are not sensitive to acuity loss and contrast sensitivity loss.
 |
 |
| Figure 3A | Figure 3B |
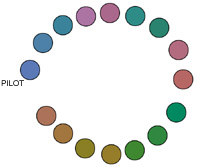
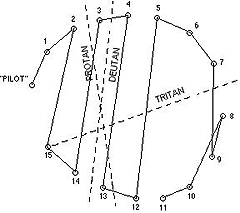
Figure 3. Deutan Defect
A. The caps are arranged so that "closely similar" caps are next
to each other.
B. Results drawn on the recording sheet show crossings in
the deutan axis.
In sorting tests, the colour defective person arranges the caps in an order different from that of a person with normal colour vision. Colours that look similar to the person with a colour defect are placed next to each other (Figures 3A and 3B).
In clinical evaluation of adult subjects the size of the stimulus should be 1.5° of angle. This means a working distance of 50 cm (19.5 in) with most tests. If the subject bends closer, the stimulus area increases. Standard evaluation is done with the small stimulus size. Subjects with mild colour vision defects may discriminate and sort colours normally when large stimuli are used. For functional purposes, it is of interest to test with large size caps as well. When testing children, it is helpful to start with the large stimuli and proceed testing with small cap sizes.
Acquired Colour Vision Defects
Colour vision defects (also called dyschromatopsias) that are caused by diseases or trauma may affect cone cells, inner retinal layers, optic nerve fibers or the visual cortex. The structural and functional changes may be patchy or diffuse and may affect vision in one eye more than in the other eye. For diagnostic purposes, the eyes are tested separately. For functional purposes, binocular measurements are more informative.
Macular lesions often cause a defect with the blue-yellow, or tritan, axis since there are fewer S-cones than L- and M-cones, and they are concentrated around the edge of the fovea. However, when the lesion is small or patchy, either there is no axis present or it varies from day to day.
Screening tests that are designed for revealing red-green defects do not pick up acquired defects in the blue-yellow axis. A few screening tests have plates for the blue-yellow defects.
Results in quantitative testing vary as a function of stimulus size. This is more pronounced in acquired colour vision defects than in congenital colour vision defects. Results from testing with small stimuli depict function in the preferred retinal locus used for fixation, whereas results from testing with large stimuli give information on colour perception in everyday life.
Colour of an adjacent surface may alter the perceived brightness and hue of nearby colour surfaces. This causes an additional confusing factor in assessing vision for ADL (Activities of Daily Living).
In diagnostic evaluation the tester should be aware of the fact that reduced retinal illuminance due to cloudiness of the cornea, lens or vitreous distorts test results. In such cases, increased illumination may decrease the degree of the defect or make it disappear. Illumination should be either natural, overcast daylight at a window facing the northern sky (in Northern Hemisphere) or artificial light with colour temperature of 6774 K (Standard Illuminant C).
![]()
![]()
![]()
[ Instructions I Paediatric Vision Tests I Vision Tests ]
This document was last modified on