8. Brain Damage Related Vision Loss

CVI, cortical visual impairment was first a term used when a child had normal looking eyes but was functionally severely visually impaired. The term cortical blindness was also used when the child could not be tested with the routine vision tests although these children rarely were functionally blind. The term CVI can also be used for the term cerebral visual impairment that is more often correct than cortical visual impairment because a great majority of these children have both cortical and subcortical lesions. Pure cortical lesions are rare.
CVD, cortical visual disability or dysfunction is a name that best describes the medical aspects of the problem. It is not impairment but capability/ability that we assess for early intervention and educational purposes. In psychology and in special education the term cognitive visual dysfunction is most often used. Some people understand this term so that cognitive visual impairment is not 'real and proper visual impairment' if visual acuity is close to normal. We should keep in mind that recognition of optotypes is one of many recognition functions, a cognitive function. In the life of young children recognition of facial features and facial expressions is far more important than recognition of abstract black-and-white forms.
Structure of visual pathways should be kept in mind when we assess children with brain damage. I recommend that everyone draws this picture as many times as is needed until it is drawn without any difficulty and the different parallel functions can be explained to parents and day care personnel and teachers.
Parallel pathways are the important feature of visual pathways. At each level of functions we have parallel functions that can become impaired one more than the other. This leads to the great variation that we see in visual impairments and explains why clinical measurements do not depict the severity of impairment and even less disabilities.
There are cone and rod cells at the level of sensory cells, magnocellular and parvocellular pathways from the retina to brain, retinocalcarine and tectal pathway, dorsal stream and ventral stream and cortical and subcortical functions. Of the many visual functions usually only two, visual acuity at high contrast, higher than ever experienced in every day life, and the size of the visual field are used to classify visual impairment. In the US the definition of 'legal blindness' means that there is plenty of 'illegal blindness' in that country, especially among those with brain damage related visual impairment.

If an infant is known to have brain damage, sensory functions are nowadays examined better than ten years ago but still functions like accommodation and use of vision in communication are not assessed, although it is well known that early interaction lays the foundation for emotional development. If brain damage is not diagnosed, cognitive visual impairment very often is misunderstood. The child is felt to be autistic and developmentally delayed because the behaviours of visually impaired children mimic those of autistic children. The causes of specific behaviours are different from those of autistic children; these children do not see the world like their healthy peers. If the typical behaviours are known by people in day care and schools early diagnosis becomes possible. The most common typical feature is variation in visual functions. Some of this phenomenon is caused by the specific loss of some visual functions. Tasks related to lost functions are performed worse than tasks related to visual functions that the child has.
If the child's intellectual development is normal (s)he learns to avoid difficult situations by using compensatory functions. If recognition of facial features and facial expressions is difficult the child cannot cope with the highly visual communication of toddlers and therefore stays with the teacher talking with her, often even functioning as an teacher's aid to master the stressful situations in communication.
To a child who is strongly dependent on auditory information the present noisy day care places are often so stressfull that the child prefers to stay in a corner or may even close him/herself in a closet to have a more pleasant play situation.
When out shopping with the parents, the child may be upset because of fear of loosing the parents in the crowd. Beaches and swimming pools are specially problematic because clothing differences are so small that recognition of parents is difficult. In Finland, where CP-children and their mothers go to sauna before exercises in the pool, 'panic reactions' occur in children (who do not recognise people) in the sauna if the mother moves to do something - and disappears in the group of nude women. These 'panic reactions' disappear if the mother wears something easily recognisable on her leg or arm. If a three year child suddenly does not see her/his mother, a panic reaction is understandable.
These children often use colours of clothing to describe persons: that girl with the red skirt, the boy with yellow cap.
If the child has increased crowding (s)he may learn letters early but does not learn to reads words longer than 2-3 letters. A 4 year old patient of mine described the difficulty well by saying that letters in longer words could not be read because 'they hug each other', which beautifully describes how the letters glide partially on top of each other. A child with 0.8 (6/9, 20/25) visual acuity with single symbols at distance, may have 0.08 (6/90, 20/250) visual acuity at near with the crowded side of my LEA SYMBOLS® test and may need to read with a CCTV. Those children whose form perception is better through 'form in motion' may wiggle the text under the CCTV to increase input through that channel - not to annoy their teachers.
Some children start to draw late, some never. They may have problems in eye-hand-coordination, in perception of complex pictures or in the structure of egocentric space.
When a child's spatial concepts are weak or distorted, orientation in space is difficult. Some children do not see the difference between shadows and thresholds and use tactile information to confirm the structure, i.e. feel with their foot or hand. In infancy this may make the infant afraid of moving from the training mat to the floor; the less than five centimetre 'cliff' is frightening high.
If the quality of the primary image is poor due to low contrast sensitivity or patchy loss of visual field, the child may get lost even in his/her own living room.
When perception of objects on a background is disturbed, the child learns to use memory to find his/her toys, cloths etc. placing them in a certain order like blind children. If somebody moves one of the items, the child may be badly upset when not finding it on its place and not noticing it less than half a meter away.
If motion perception is poor the child may have peculiar fears of small dogs but not big dogs. Small dogs move quickly from place to place and if the movement is not perceived, the dog appears here and there and the child can never know where it is going to appear next. These children later have great problems in traffic. Even if they learn to conclude that a car that a moment ago was in front of a house and now is in front of another house, must be moving, they do not experience the essential element of relative and real movements.
Many children with brain damage related visual impairment are diplomatic in asking for help in tasks that they cannot do themselves. This functions well at home and in the nursery school but when the child comes to school this useful technique is no more allowed, which adds to the frustrations experienced in a new place and new group of children.
Cognitive vision tests are used by neuropsychologists who should first examine the quality of visual information used in the test situations. To make such assessment quick and easy I have designed half a dozen tests that assess the early phases of higher visual functions. We have already discussed the Heidi Expressions test, the LEA 3-D Puzzle, and visual acuity tests to diagnose increased crowding (for details see slide 50). There are two paediatric modifications of neuropsychologic tests, the LEA Rectangles and the LEA Mailbox that should be used before the more complex tests.
LEA Rectangles is an educational plaything derived from Efron's rectangles to assess vision for perception of sizes and LEA Mailbox is used to assess vision for perception of orientation of lines.
Motion perception can be observed during measurement of grating acuity with the LEA GRATINGS and during the Hiding Heidi test, when rolling balls of different sizes and observing the child's behaviour when figure-in-motion is shown.
Vision for perception of orientation of lines has two components, information for the hand movements in the parietal lobe and for picture perception in the inferotemporal lobe. To observe the first function the child is asked to drop a card through the slot of the LEA Mailbox. The card is given to the child in another orientation than that of the slot. If the orientation of the slot is perceived by the child the card is turned in correct orientation before it has moved half of the distance to the slot (dorsal stream function). If the orientation is not perceived the card hits the 'mailbox' in the original orientation and does not get through the slot. In that case dropping of the card through the slot needs to be trained to find out whether this function is trainable.
The other part of the test is more difficult because younger children do not understand when we ask them to show the orientation of the slot at a distance of more than half a meter without moving the card closer (ventral stream function). Often another adult is needed in this test situation. The adult pretends not to know when the orientation of the card is correct, turns the card in varying orientations and asks the child whether the card is in the same orientation as the slot. If a child cannot purely visually perceive the orientations of lines, drawing lines is often difficult and drawing angles makes no sense.
{kind=link}
LEA Mailbox can be used also during an office visit. It does not take much time and reveals the quality of important basic visual functions.
LEA Rectangles follow the principle suggested by Efron: The total area of the rectangles is constant so for example luminance reflected from the surface cannot be used to perceive size differences, the differences in length must be seen.
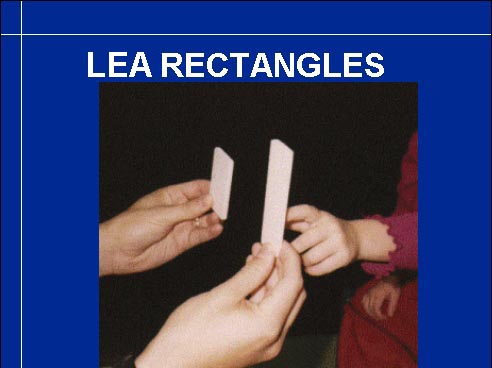
A three year old child can tell which of the two rectangles is the longer one. If not, the rectangles are studied using haptic and tactile information. If the child can learn that the rectangle that is felt outside the other rectangle is the longer one, the child has a correct nonvisual concept of length. If the child still cannot tell which of the two rectangles is the longer one when looking at them, the child has a specific loss of vision for size differences (ventral stream function).
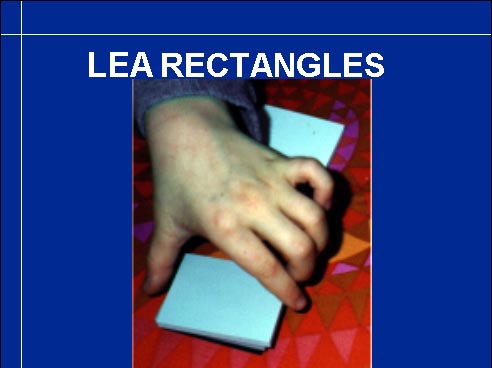
To examine the corresponding function in the parietal lobe we ask the child to grasp the rectangles one by one and arrange them in a neat row. By observing the distance between the thumb and the forefinger we detect whether the visual information guiding the hand movements is correct.
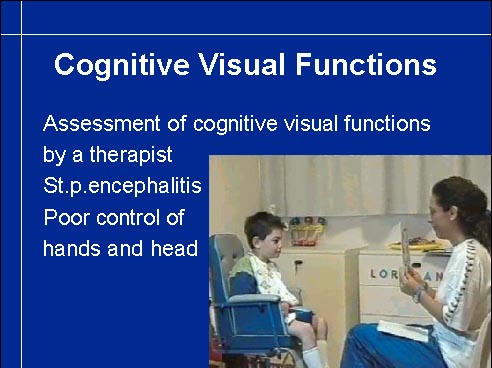
Video
These very short sequencies from the first assessment of vision after severe brain infection clearly shows that the tests can be used by a therapist trained in vision therapy and that communication is possible even if the child has lost his voice, has poor head control and very little functions in the arms and hands. His eye movements were normal so he uses gaze to point although he tries to point with his hand as well and nods for 'yes'.
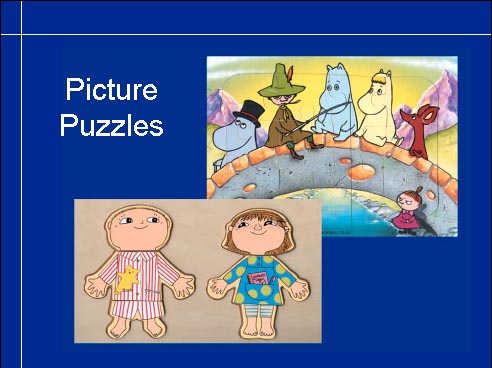
Picture puzzles are useful in assessing the child's ability to use parts to build a complete picture. Some children who cannot see the complex picture may be able to place the puzzle pieces so that they fit in their places but are not connected with the content of the picture. The child sees forms and their orientation but cannot use that information to interpret pictures. Puzzles need to be both very simple and more complex to reveal which step in solving the problem is the most inhibiting one.