Vision Care 3 years to 10th grade
[ 1-27 ]|[ 28-50 ]|[ 51-75 ]|[ 76-100 ]|[ 101-128 ]

Video 6
Before testing face recognition, we need to find out that the image quality is good enough to allow comparison of pictures. When the girl was asked to match the pictures, she had no difficulty, i.e. the incoming visual information is of good quality. Her corrected visual acuity and contrast sensitivity are close to normal and color vision is quite normal.

When she was asked to tell who the children were, during the first testing she was unable to name these children whom she saw each day. However, when we made this video sequence for teaching a few weeks later she surprised us by knowing the names of each child. Since we knew that she had not recognized them the same day, I asked how she knew the names. She explained that at each of the cards there were small differences, one corner darker than in other cards, a bit more hair showing than in the other cards etc. Like many other intelligent children with CVI, she used whatever details there were to remember the name related to that card. She did not recognize the faces. Test cards do not function well more than once if the names are told to the child at the end of testing.
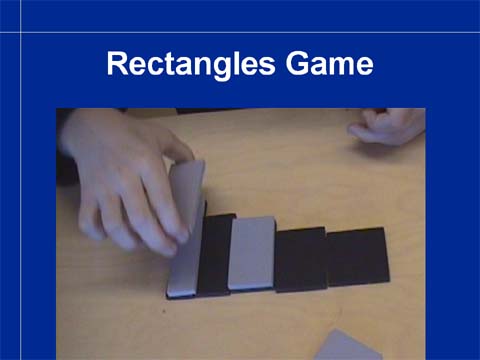
Perception of the length of lines is related to groups of cells in V1 that are active if a line ends within their receptive fields. If these cells do not have normal connection to the cell groups in the inferotemporal cortex that are responsible for coding for length of lines then the length of lines is not perceived. If the information flows to the parietal lobe and can be used for planning of hand movement, then the distance between the fingers is correct before grasping the test rectangles although the child has just demonstrated that (s)he does not see the length. These two seemingly same functions are localized in different neural networks so that one function can be lost and the other may be normal.
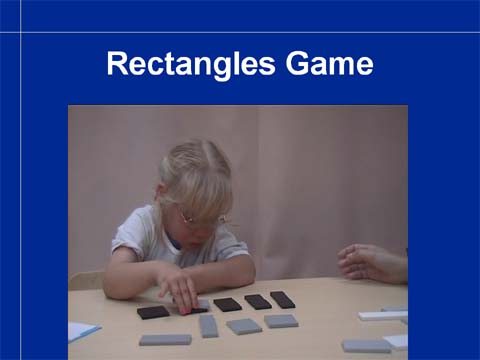
When testing children with increased
crowding,
it is fair to place the rectangles farther apart.
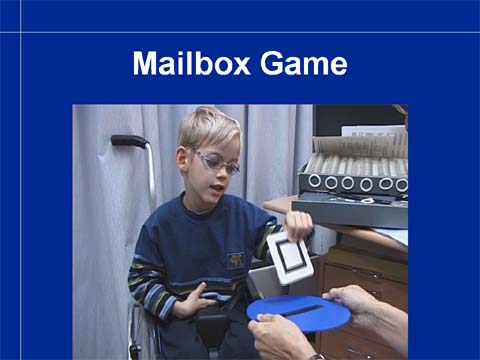
Direction of lines is another early phase in the analysis of incoming visual information.
It is assessed both as the ability to turn the card in correct orientation before it touches the “Mailbox” (parietal lobe function) and how exactly the child can perceive orientation of two lines being parallel or slightly nonparallel (inferotemporal lobe function).
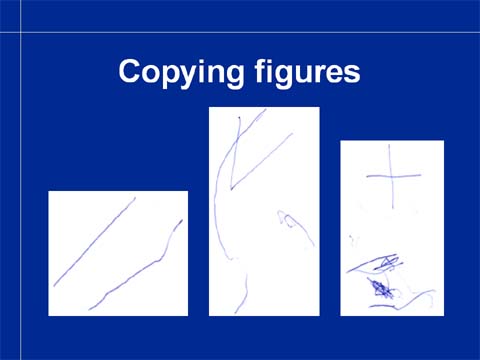
Copying basic figures may reveal losses of function in the early analysis of visual information or in the use of visual information for hand functions. This child can copy parallel lines reasonably well (the child has motor problems) but drawing an angle or a cross did not result in a form that would resemble the model figure. It was drawn while the child was watching, which is an important detail in testing. In the picture there are two trials of drawing both the angle and the cross. This child could tell what his figures were not like mine but his “hand did not do” what he wanted to do (i.e. he had the idea of general planning what to do but the not the planning functions for the detailed performance).
Slide 107.
Slide 108.
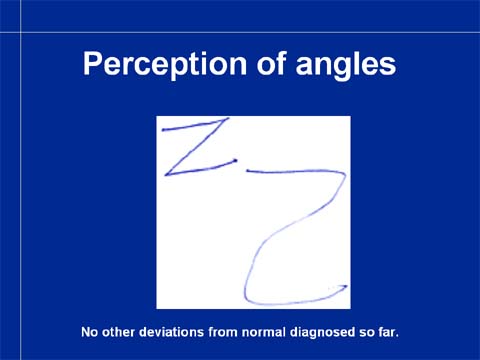
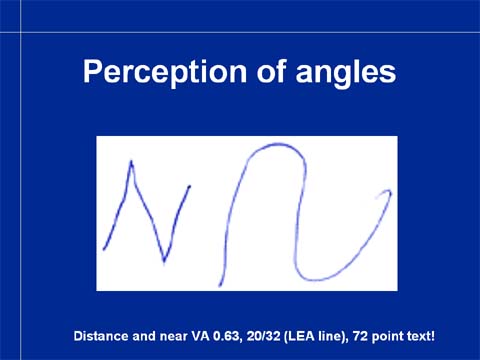
Some children do not perceive the crossing point of lines in angles but draw V like a U. These two slides depict letters drawn by two children who insist that what they have drawn is exactly the same as what the teacher drew. One of them has visual acuity 0.63 but prefers text size 72 points, in the other child only this visual function seems to be impaired. These children may become aware of the angle, if the therapist/parent draws with the child and demonstrates that the line stops and then goes in the other direction starting from that stop point. The child may still be unable to see the difference but may be able to use motor memory to draw letters correctly. In geometry this difficulty requires careful assessment so that teaching avoids such visual concepts that the child does not have and uses teaching techniques for blind children, when needed.
Slide 109.
Slide 110.
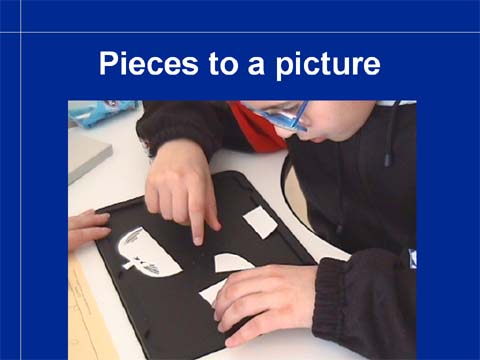
Some children cannot figure out how to compose even the simplest picture of a few pieces. Puzzles are an important part of vision training in preschool functions and good diagnostic tools for assessment of CVI.
Slide 111.
Slide 112.
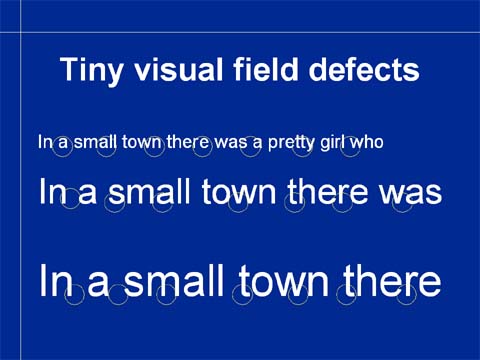
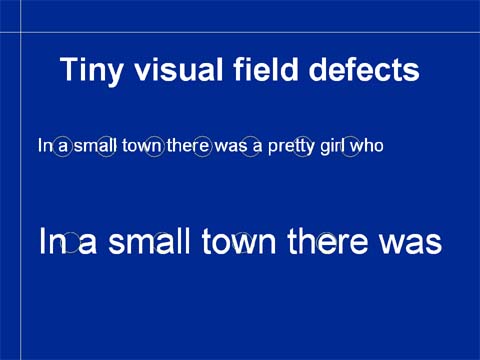
When errors in reading are not typical to dyslexia, they could be caused by tiny scotomas in the central visual field. This is easy to test at school: enlarging the text first changes the type of errors and at a certain size errors disappear. At that size the scotoma covers such a small part of a letter that the letter can be seen clearly enough. The child may notice that fixating the gaze in different parts of the text may make it clearer (at the lower upper edge of the letters in this case because the scotoma then fells on the lower part of the letters that are less important for recognition than the upper parts).
When you measure normal visual acuity in a child with reading problems, ask the teacher to check reading with different sizes of text before other more expensive investigations are started.
Slide 114.
Slide 115.

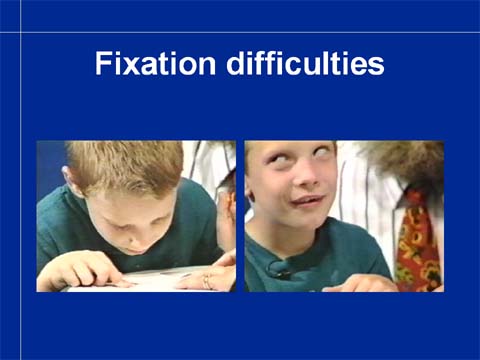
Children with CP may have major difficulties in fixation and accommodation. If the motor problems are as severe as in these two children, they are visually impaired and require auditory teaching techniques and modifications in learning materials irrespective from what their visual acuity values are.
In the assessment of visual functioning of children, especially those with motor impairments, we shall carefully assess the motor functions. If the child has poor head control or posture, the effect of supporting the child in different ways and facilitating the motor functions is a part of the basic assessment.
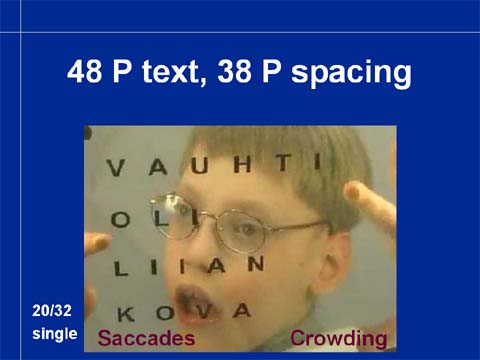
Saccades, rapid eye movements from one fixation to another are the motor function that we use when scanning environment or a page of a newspaper. They are essential for normal reading. Each gaze shift is composed of several brain functions: 1. a visual map is created and the distance from the present fixation to the next fixation is “measured”, 2. this information is passed to the motor planning of eye movements where the motor task is defined, 3. a command is sent to all twelve eye muscles, 4. before the movement can start, the gaze must be detached from the present fixation, then the movement follows, 5. gaze land on the next point of fixation and is attached there. Any of these motor functions or the visual map may be defective. If these movements are not automatic they become much slower and inexact.
Slide 118.
Slide 119.

Slide 120.

Slide 121.
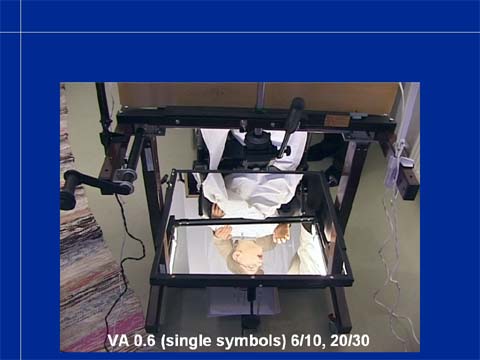
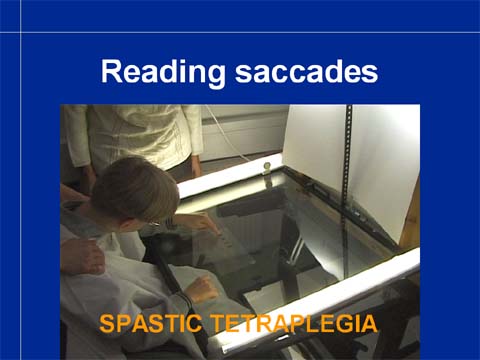
Reading saccades of children with poor head control can be documented on video film using this kind of equipment: the text is written on transparent film and placed on glass table; the child wears white apron that gives white background to the text and is supported by a therapist or assistant to sit comfortably; via a mirror the child’s eye movements can be recorded on the other side of the equipment.
Video 7
Although the eye movements cannot be measured, we get enough information to understand how difficult it would be to try to read with these motor functions. This child can fixate when he points with his finger on the letter to be read. The hand movements are irregular so he needs help in finding the correct place. When there is a letter that is difficult to pronounce, like the letter V in the last word, fixation is interrupted, the head turns back, the eyes go up and finding back to the point to read takes time. If reading requires this much of concentration, how much is left over for remembering the content of the text?

Children who cannot talk are a real challenge. Most of them have much to say. When motor functions are poorly controlled, skillful facilitating of the movements may make it possible for a child to point on the sentence that he would like to say.
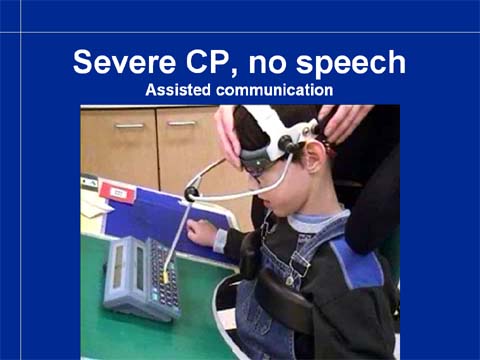
A more advanced technique is possible when the child has learned to write. Gentle support of the head allows the child to write with a head-stick.

Video 8
Among the children who have severe CP there are many who are very difficult to assess. Often their functional level is underestimated because we do not notice the short moments when the child is able to look at the object that (s)he wants to look at. In the still picture from the video sequence that you can play next, this girl seems to look at one of her favorite objects with eyes well aligned. She looks quite normally functioning. When you now play the video you see that that moment last less than two seconds. Most of the time the eye and head movements are uncontrolled. Despite these major motor difficulties she was learning to read at the time of this recording.

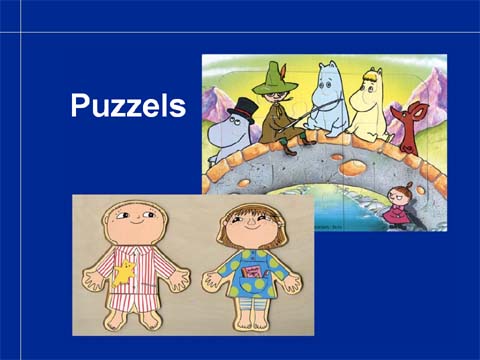
I would like to end my lecture on children with special needs with this picture of a puzzle that a child with CVI had completed. When you first look at it, it looks reasonably normal (as do many children with CVI). The more you study it the more details you find that do not really match. However, also this kind of information is useful for learning but learning may take much more time and some things that teachers and other adult people say, may not make sense.
As a summary, our vision services at preschool and at school cover vision screening for amblyopia and other forms of impaired vision in the age group 3 years to second grade, screening for refractive errors that may decrease vision comfort at school work and assessment of vision of children with special needs.
Slide 128.
